 Tweet
Tweet
bump this
-
-
une question pour tous, mais le regard de Vibran62 m'importe: vu le fric mis sur la table et la nature de ce virus, connue de beaucoup, pourquoi avoir choisi un vaccin intramusculaire et pas un vaccin nasal, donc muqueux?

Cette question, va avec une autre, la contamination buccale, exemple certains sushis, ne peut permettre une forme de contamination intestinale , donc induire une immunit? muqueuse ?
Une derni?re : la recontamination, ? but th?rapeutique, de selles contamin?es peut ou pas ?Comment
-
Bertrand - Je ne sais pas pourquoi ils ont choisi intramusculaire vs muqueux; peut-?tre parce que cette voie est g?n?ralement connue pour produire des r?ponses immunitaires plus fortes. Je suis ? peu pr?s s?r d'avoir vu des recherches r?centes sur un syst?me d'administration de vaccin autre que l'injection - je pense que via la forme d'une dose orale, et si elles peuvent produire cela et que cela soit s?r et efficace, cela doit ?tre un meilleur id?e. Cela supprimerait les besoins d'injection et les infrasturctures n?cessaires pour les injections en termes d'aiguilles et d'individus qualifi?s pour administrer une injection.
En ce qui concerne les modes f?caux de transmission virale - nous savons que le virus est isol? du tractus gastro-intestinal, il doit donc ?tre possible de la m?me mani?re que le norovirus est transmis. Je ne pense pas que cela ait ?t? un probl?me important et n'a donc pas attir? beaucoup d'attention, mais je m'interroge sur les r?centes mesures prises par la Chine pour exiger des pr?l?vements anaux. Peut-?tre que l'accent mis sur la pr?sence de virus nasaux dans les tests pr?c?dents signifie qu'ils ont une variante qui se transmet mieux de cette mani?re en Chine? Je ne suis pas s?r des preuves ? l'appui ici.
J'esp?re que Giggle translate a fait un travail raisonnable avec ma r?ponse ? vous! -
Merci, je pensais ? ceci
Yl?-Herttuala explique que si les vaccins intramusculaires produisent des anticorps de type immunoglobuline G dans le sang, les vaccins nasaux produisent ?galement des anticorps de type immunoglobuline A qui prot?gent les muqueuses. ? Nous supposons que cela peut ?galement emp?cher les personnes qui ont re?u le vaccin de transmettre le virus ?, a-t-il d?clar?
-
-
medRxiv
An observational cohort study on the incidence of SARS-CoV-2 infection and B.1.1.7 variant infection in healthcare workers by antibody and vaccination status
Sheila F Lumley, Gillian Rodger, Bede Constantinides, Nicholas Sanderson, Kevin K Chau, Teresa L Street, Denise O?Donnell, Alison Howarth, Stephanie B Hatch, Brian D Marsden, Stuart Cox, Tim James, Fiona Warren, Liam J Peck, Thomas G Ritter, Zoe de Toledo, Laura Warren, David Axten, Richard J Cornall, E Yvonne Jones, David I Stuart, Gavin Screaton, Daniel Ebner, Sarah Hoosdally, Meera Chand, Oxford University Hospitals Staff Testing Group, Derrick W Crook, Anne-Marie O?Donnell, Christopher P Conlon, Koen B Pouwels, A Sarah Walker, Tim EA Peto, Susan Hopkins, Timothy M Walker, Nicole E Stoesser, Philippa C Matthews, Katie Jeffery, David W Eyre
doi: https://doi.org/10.1101/2021.03.09.21253218
This article is a preprint and has not been certified by peer review [what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.
AbstractFull TextInfo/HistoryMetrics Preview PDF
Abstract
Background Natural and vaccine-induced immunity will play a key role in controlling the SARS-CoV-2 pandemic. SARS-CoV-2 variants have the potential to evade natural and vaccine-induced immunity.
Methods In a longitudinal cohort study of healthcare workers (HCWs) in Oxfordshire, UK, we investigated the protection from symptomatic and asymptomatic PCR-confirmed SARS-CoV-2 infection conferred by vaccination (Pfizer-BioNTech BNT162b2, Oxford-AstraZeneca ChAdOx1 nCOV-19) and prior infection (determined using anti-spike antibody status), using Poisson regression adjusted for age, sex, temporal changes in incidence and role. We estimated protection conferred after one versus two vaccinations and from infections with the B.1.1.7 variant identified using whole genome sequencing.
Results 13,109 HCWs participated; 8285 received the Pfizer-BioNTech vaccine (1407 two doses) and 2738 the Oxford-AstraZeneca vaccine (49 two doses). Compared to unvaccinated seronegative HCWs, natural immunity and two vaccination doses provided similar protection against symptomatic infection: no HCW vaccinated twice had symptomatic infection, and incidence was 98% lower in seropositive HCWs (adjusted incidence rate ratio 0.02 [95%CI <0.01-0.18]). Two vaccine doses or seropositivity reduced the incidence of any PCR-positive result with or without symptoms by 90% (0.10 [0.02-0.38]) and 85% (0.15 [0.08-0.26]) respectively. Single-dose vaccination reduced the incidence of symptomatic infection by 67% (0.33 [0.21-0.52]) and any PCR-positive result by 64% (0.36 [0.26-0.50]). There was no evidence of differences in immunity induced by natural infection and vaccination for infections with S-gene target failure and B.1.1.7.
Conclusion Natural infection resulting in detectable anti-spike antibodies and two vaccine doses both provide robust protection against SARS-CoV-2 infection, including against the B.1.1.7 variant.
...
Comment
-
COVID-19 and IL-6: Why Vitamin D (probably) helps but tocilizumab might not
https://www.sciencedirect.com/scienc...849?via%3Dihub
l'?tat des lieux du su concernant cette vitamine est accessible ou ?
Comment
-
bump thisComment
-
l'on m'a fait lire ceci :
un texte port? , par des femmes et pourtant humiliant pour toutes celles qui ont un cerveau ou qui sont dans des fonctions ou la parole n'est pas possible ...Comment
-
New University of Colorado study finds COVID 'super carriers' are responsible for bulk of infections
By Seth Klamann The Denver Gazette Mar 15, 2021 Updated 10 hrs ago
...
The study, which has not yet been published in a peer-reviewed journal, found that 2% of people with COVID carried 90% of the virus in circulation. In other words, one of the study's authors said, if you were to add up the viral load of 100 people, nearly all of that viral load could be accounted for in just two people.
"A higher rate of spread by viral super-carriers would be consistent with recent contact tracing analyses suggesting that 80-90% of infections are spread by 10-20% of infected individuals," the authors wrote, referencing studies that looked at spread in China and Hong Kong.
....
?The takeaway from these studies is that most people with COVID don?t get other people sick, but a few people get a lot of people sick,? Sara Sawyer, a specialist biology professor and senior author of the study, said in a statement. ?If you don?t have a viral super-carrier sitting near you at dinner, you might be OK. But if you do, you?re out of luck. It?s a game of roulette so you have to continue to be careful.?
...
https://gazette.com/news/local/new-u...5245f249c.html
--------------------------------------------------------
medRxiv preprint doi: https://doi.org/10.1101/2021.03.01.21252250; this version posted March 5, 2021.
...
Just 2% of SARS-CoV-2-positive
individuals carry 90% of the virus
circulating in communities
Abstract
We analyze data from the Fall 2020 pandemic response efforts at the University of
Colorado Boulder (USA), where more than 72,500 saliva samples were tested for SARS-CoV-2
using quantitative RT-PCR. All samples were collected from individuals who reported no
symptoms associated with COVID-19 on the day of collection. From these, 1,405 positive cases
were identified. The distribution of viral loads within these asymptomatic individuals was
indistinguishable from what has been previously reported in symptomatic individuals.
Regardless of symptomatic status, approximately 50% of individuals who test positive for
SARS-CoV-2 seem to be in non-infectious phases of the disease, based on having low viral
loads in a range from which live virus has rarely been isolated. We find that, at any given time,
just 2% of individuals carry 90% of the virions circulating within communities, serving as viral
?super-carriers? and possibly also super-spreaders.
...
The concentration of a majority of the virus in a small fraction of the population at a given
time is a critical observation with actionable conclusions. Community screening to identify viral
super-carriers within pre-symptomatic and asymptomatic stages of disease will be important,
since these individuals will continue to sustain and drive the epidemic if not located. Finding viral
super-carriers will have a disproportionately large impact on curbing new COVID-19 infections,
yet individuals without symptoms don?t tend to seek out testing so screening will need to target
healthy populations. Modeling approaches show that one of the most important factors in
screening for SARS-CoV-2 will be the speed with which infected people receive their test results
(also referred to as turnaround time) [50]. The longer it takes for people to receive their results,
the more time goes by where they might unwittingly infect others. Therefore, it is imperative that
we find virus super-carriers, and inform them of their infection status in a way that is fast, easy,
and accessible. Although sensitivities vary between current monitoring and diagnostic
paradigms, all are more than capable of finding the majority of infected individuals and the vast
majority of infectious virions (Figure 3).
https://www.medrxiv.org/content/medr...52250.full.pdfComment
-
Although this is only a preprint it is exactly what I would expect. Mina's calls for a very basic and very low cost antigen based test is based on the fact that the very high viral loads found in the day or two before and after symptom onset are likely to account for the bulk of infections. A very cheap, but not particularly sensitive, self administered test giving immediate results is far more effective at picking these up than an unnecessarily sensitive PCR test that may not return a result until after the peak infectious period is past. PCR is great for clinical testing but not a good way of stopping spread. -
JJackson - this is definitely the way the UK seems to be heading with its widespread use of rapid flow testing 2 x weekly in schools and workplaces. Free tests have been made available to families of schoolchildren and workplaces. It seems to me this is the way forward and if they can be mass produced at low enough costs for self-testing, it is the way forward out of lockdown and restrictions IMHO.
-
-
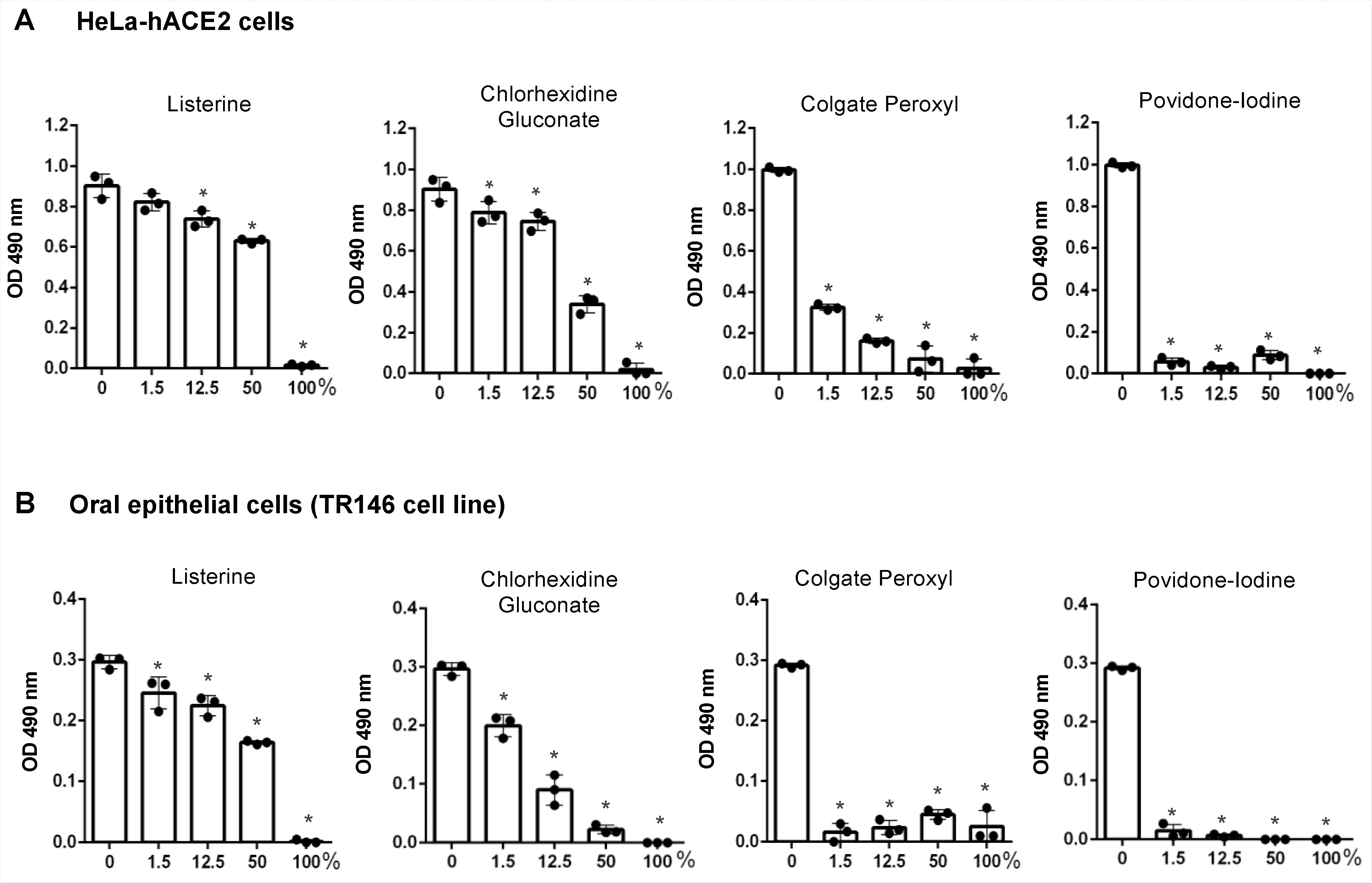
Another good article about mouthwash research.
_____________________________________________
Ask Congress to Investigate COVID Origins and Government Response to Pandemic.
i love myself. the quietest. simplest. most powerful. revolution ever. ---- nayyirah waheed
"...there’s an obvious contest that’s happening between different sectors of the colonial ruling class in this country. And they would, if they could, lump us into their beef, their struggle." ---- Omali Yeshitela, African People’s Socialist Party
(My posts are not intended as advice or professional assessments of any kind.)
Never forget Excalibur.Comment
-
France -
Translation Google
CQFD
Covid: why self-tests could help fight the epidemic
The High Authority for Health (HAS) on Tuesday gave the green light to the use of these nasal tests carried out at home without the help of a professional. Operation, efficiency, context? Update on this new tool, which could soon help to curb the epidemic.
By
Yann Duvert
Posted on 18 March 2021 at 11:10 Updated on 18 March 2021 at 13:58
After the green light from the High Authority for Health, France is preparing to strengthen its arsenal against the Covid-19 epidemic. Unless surprised, the government should allow home tests, also called self-tests.
1) What is it?
The basic principle is the same as for antigenic tests, which are currently possible in pharmacies. But as the name suggests, the self-test does not require the presence of a healthcare professional and can be used by anyone over the age of 15.
Its operation is simple, since it suffices to push the swab 3 or 4 cm deep, and not to the back of your nose. After having rubbed the walls, the Cotton Swab is immersed in a tube filled with a solution. If the test is positive, a colored strip appears. The result is usually available in less than 30 minutes.
2) How effective are they?
Work is still ongoing to determine their actual effectiveness. The first data are encouraging, however, with clinical sensitivities of around 80 to 95% in symptomatic patients, according to the HAS. On the other hand, the reliability could be between 50% and 60% for people without symptoms, who are precisely the target audience for these tests. In addition, their use by patients themselves and not by professionals can potentially reduce their effectiveness if the procedure is poorly performed.
A positive result must imperatively be confirmed by a PCR test.
As with the nasopharyngeal antigen tests, a positive result must imperatively be confirmed by a PCR test, the reliability of which is higher and which will make it possible to "trace" the epidemic.
3) In what context can they be useful?
Self-tests could allow better monitoring of the epidemic. Less reliable than PCRs, however, they have a triple advantage: ease of access, ease of use, and almost immediate results. Their use is therefore recommended in the private sphere, for example before a family reunion - which in no way exempts the participants from the usual barrier gestures.
4) Where can we get it?
The self-tests will be available in pharmacies, once the government has given its approval. The latter will also have to determine whether these tests will be covered by Social Security, at least partially.
According to the Director General of Health, J?r?me Salomon, their marketing could also be authorized in supermarkets. The heavyweights in the sector have also taken the lead: Carrefour has already announced that it has ordered a million tests, while its competitor Syst?me U has expressed its interest.
With AFP
Comment
-
Not related to any posts on this thread.....
Please no name calling. We do not bash here. Many of us disagree with various experts, famous peeps, etc. If you do not agree, just say...."I do not agree for the following reasons....". Listing someone's accomplishments, or lack thereof, is fair. Their past papers, verified quotes, their resume...all fair.
Just no name calling....please.....
Thanks!
Comment
-
So today I signed up for a Moderna shot. I had no choice. A household member has jury duty in two weeks that they have not been able to be excused from. I am high risk for COVID-19 and Florida is continuing to be a national hot spot for variants. link I believe the UK variant is more contagious and more deadly than "regular" COVID-19. On top of this, no one expected the Spring Break surge hitting Florida right now. In my opinion this is a huge spreader event. And I am in the middle of it. linkOriginally posted by sharon sanders View Post
I think in a pandemic you have to be constantly re-evaluating your personal situation. Things change. While my plan was to wait until June, I assess that my risk has exponentially increased with the jury duty requirement for a person in my household. They are still going to try to re-schedule still, but since they already re-scheduled once, those prospects look dim. The county states that these jury assignments are only for one day. How can that be? I am highly doubtful that jurors can be guaranteed a limit of a one day trial. What kind of justice is that? I suspect they say this so people will show up at all. We discussed getting a hotel room for the family member but they are also high risk and not vaccinated at this time. A hotel will only increase their risk further with the lobby, central halls, elevators, food, so they will have to come home each night if they are selected for duty.
Anyway, this jury thing pushed me over the edge.
I am neither pro-vaccine or anti-vaccine. I think my long history of posts on this site demonstrates this. Some years I get the flu shot, some years not. I vaccinated my children when they were small because we always lived in a large, dense metro area, but I was not a parent who rushed to the doctor for every sniffle. I appreciate modern medicine but I also think that natural medicines are very important to incorporate into our lives.
This is not medical advice. If you have any questions about vaccines, consult your medical provider.Comment
-
I just received a very nice message about my family member's autoimmune disease and obtaining a doctor's note to be excused from jury duty. I am fairly sure we could get a note (although my family member is not totally incapacitated). This family member has two specialists that they see for this condition. The issue, we discovered this week, is that only a judge can authorize an additional 6 month deferral. We are not sure what the procedure is to do this. My family member gave up and is going to get their first vaccine shot this Saturday. That will be exactly 10 days to the report date. We do not think a vaccine is any kind of "cure". It most certainly is not. While we might get sick, our hope is that it is enough to keep us from dying. I do not think we can avoid COVID-19 forever. So.....groan. Thank you to everyone who follows FluTrackers. We love all of you. -
The data show that 14 days is quite a sharp cutoff point in there is little or no protection up to that time after which the protection ramps up fairly quickly. Given the enormous number of people who have now been vaccinated, and the absence of any detectable problems against the background despite very careful follow up, I can not see any reason not to get vaccinated - assuming you have no prior history with other vaccines or anaphylaxis. No vaccine is 100% without risk but given the known risks of a COVID infection the benefits clearly vastly outweigh the risks in the middle of a pandemic. -
My family member's autoimmune disease problem is that it is too active. Maybe they will have a quicker response than 14 days. They have only been eligible to get a shot for two weeks. Most states took almost three months to drop the age eligibility below 65. So far I am not having any adverse reaction. I had a sore spot at the injection site for a day. The shot itself was nothing.
-
-
Maintenant qu'il est admis que la faute est partag?e, chino am?ricaine , on va peut ?tre, si tout le monde, sait se tenir avancer.
Donc, avec tout le respect pour ce Monsieur : faire financer ce qui ne doit pas ?tre, cela ?tait b?te . Mais pour moi, il a ?t? b?te une deuxi?me fois. Alors que l'argent ?tait sur la table pourquoi ne pas avoir choisi l'option vaccin muqueux ?
Je pose cette question, ? dessein, sur ce post, car je voudrais savoir si les chinois ont un vaccin muqueux ?
Comment
-
I do not know the status of a nasal vaccine in the US. I have no idea what the China government is doing in this regard. -
dont
mais surtout ceci

le regard de Vibran sur l'?tat des lieux en chine et ailleurs sur cette voie me semble important , mais essayer d'entrevoir pourquoi elle n'a pas ?t? choisi en premier aussi ...
-
Nasal Spray Of Covid Vaccine May Be Next: Oxford Reportedly To Test AstraZeneca Version
Mar 25, 2021,11:37am EST
-
-
bien,
"The Ministry of Foreign Affairs and the National Administration of Traditional Chinese Medicine will jointly hold the "Forum on Traditional Chinese Medicine and International Cooperation to Fight Against COVID-19 Pandemic" in Beijing on March 30. Vice Premier Sun Chunlan of the State Council will address the event via videoconference."
Une enqu?te peut ?tre v??ue comme un viol . Visiblement l'O.M.S a besoin d'une profonde r?forme, notamment au niveau du vocabulaire. Ce rapport aurait du ?tre pr?sent? comme une d?marche retour d'exp?rience. Ce texte chinois , seul est ensuite soumis aux vis des partenaires de l'O.M.S.
Ce qui importe ? certains, dont moi, c'est d'abord de lire les versions chinoises, des d?marches retour d'exp?rience sur les situations m?dicales, humaines et animales*, puis pharmaceutiques.
Qu'il y ait des escrocs aux USA, tout le monde l'admet , mais visiblement cette particularit? existe aussi en Chine et visiblement ? des niveaux politiquement haut ( cel asemble une tradition de demettre des personnages important, ce n'est pas un jugement, mais un fait )
Le 30 mars devait ?tre la f?te du retour en gr?ce de la m?decine traditionnelle chinoise. J'ai peur que cela ne soit pas le cas, ce que je d?plore .
- qui se souvient de ces collyres aux fientes de chauve -souris ?
- qui se souvient de cet enfant hyper ob?se suite ? l'usage de produits dit traditionnels?
- les wikip?dias abordent bien des aspects : https://fr.wikipedia.org/wiki/Sant%C...4te_d%27Ivoire
Pour aller plus loin, on a essay? de nous vendre pour un rhume , une technique de gestion , du C.D.C chinois , bas?e sur les contraintes et la vaccination de masse. Sauf que nous ne sommes pas des poules d'une part d'autre part , on sait g?rer les influenzas animaux, d'autre mani?re qu'en Chine ... Il peut donc coexister des m?thodes de gestion diff?rentes, sauf qu'elles doivent ?tre d?crites avec leurs r?sultats et inconv?nients .
Ce rapport , recueil des d?marches retour d'exp?rience, chinoises, devrait aborder et ou valider trois points :
- l'homme** vie avec des coronavirus depuis la nuit des temps. Tout comme l'animal, donc les ?tats des lieux des sus locaux, devraient ?tre partag?s.
- l'?pid?miologie doit introduire le mot synd?mie au niveau de l'O.M.S en indiquant quand cela doit ?tre en usage .
- la vaccination efficiente pour les coronavirus doit ?tre une vaccination muqueuse. Si les experts chinois, ne sont pas capable, ? ce stade, d'?crire cela , comment les respecter ?
* il y a la version officielle et l'?tat. Mais, par exemple, des sangliers qui franchissent la fronti?re, idem pour les produits de m?decine traditionnelle en donne une autre...
** il me semble que la technique normale de gestion soci?tale de l'?mergence de l'immunit? collective plus ou moins efficace semble d?sormais connueComment
-
Nous sommes le 30, donc le texte du discours ?voqu? :
"The Ministry of Foreign Affairs and the National Administration of Traditional Chinese Medicine will jointly hold the "Forum on Traditional Chinese Medicine and International Cooperation to Fight Against COVID-19 Pandemic" in Beijing on March 30. Vice Premier Sun Chunlan of the State Council will address the event via videoconference."
est accessible ?Comment



Comment