 Tweet
Tweet
Source: Eurosurveillance.org, full text: http://www.eurosurveillance.org/View...rticleId=19760
Eurosurveillance, Volume 16, Issue 1, 06 January 2011
Rapid communications
Virological analysis of fatal influenza cases in the United Kingdom during the early wave of influenza in winter 2010/11
J Ellis ( )<sup>1</sup>, M Galiano<sup>1</sup>, R Pebody<sup>1</sup>, A Lackenby<sup>1</sup>, CI Thompson<sup>1</sup>, A Bermingham<sup>1</sup>, E McLean<sup>1</sup>, H Zhao<sup>1</sup>, S Bolotin<sup>1</sup>, O Dar<sup>1</sup>, J M Watson<sup>1</sup>, M Zambon<sup>1</sup>
)<sup>1</sup>, M Galiano<sup>1</sup>, R Pebody<sup>1</sup>, A Lackenby<sup>1</sup>, CI Thompson<sup>1</sup>, A Bermingham<sup>1</sup>, E McLean<sup>1</sup>, H Zhao<sup>1</sup>, S Bolotin<sup>1</sup>, O Dar<sup>1</sup>, J M Watson<sup>1</sup>, M Zambon<sup>1</sup>
<hr class="Centre_divider"> Citation style for this article: Ellis J, Galiano M, Pebody R, Lackenby A, Thompson C, Bermingham A, McLean E, Zhao H, Bolotin S, Dar O, Watson JM, Zambon M. Virological analysis of fatal influenza cases in the United Kingdom during the early wave of influenza in winter 2010/11. Euro Surveill. 2011;16(1):pii=19760. Available online: http://www.eurosurveillance.org/View...rticleId=19760
Date of submission: 31 December 2010 <hr class="Centre_divider">
<!-- Article start --> The 2010/11 winter influenza season is underway in the United Kingdom, with co-circulation of influenza A(H1N1)2009 (antigenically similar to the current 2010/11 vaccine strain), influenza B (mainly B/Victoria/2/87 lineage, similar to the 2010/11 vaccine strain) and a few sporadic influenza A(H3N2) viruses. Clinical influenza activity has been increasing. Severe illness, resulting in hospitalisation and deaths, has occurred in children and young adults and has predominantly been associated with influenza A(H1N1)2009, but also influenza B viruses.
<hr> Introduction
The onset of this winter season in the northern hemisphere is associated with more uncertainty than usual about which influenza viruses are likely to circulate and predominate, given the varying proportions of different virus strains circulating in the southern hemisphere between June and September 2010 [1]. Notably, influenza A(H3N2) predominated over influenza A(H1N1)2009 in several countries, e.g. South Africa and Chile. The second wave of the pandemic in the United Kingdom (UK) during the winter season of 2009/10 was almost exclusively associated with circulation of influenza A(H1N1)2009 [2]. Serological evaluation in the UK of population immunity to the pandemic strain after the second wave suggested that susceptibility was lowest in younger age groups (<15 years), with significant remaining susceptibility in the age group of 15?44 year-olds [3]. In view of the importance of children in the transmission of influenza A(H1N1)2009 [4], and the limited remaining susceptibility within this group, the probability of extensive morbidity in this age group associated with this strain in winter 2010/11 was considered unlikely in the absence of significant antigenic change in the pandemic virus. The extent, however, to which influenza A(H1N1)2009 would predominate over influenza A(H3N2) and cause illness in the remaining susceptible children and younger adults was unknown.
Investigations
Virological surveillance in the UK operates through hospital laboratories in secondary care and community-based schemes. Specimens containing influenza virus from community, hospitalised and fatal cases are forwarded to the UK National Influenza Centre for further characterisation. Samples are also received directly from sentinel primary care physicians participating in virological surveillance schemes in the community [5]. An antigenic typing profile is developed for each virus isolate and compared with influenza vaccine and reference strains. Genotypic and, where appropriate, phenotypic antiviral susceptibility analyses are performed on influenza-positive clinical material and/or virus isolates. Genetic characterisation is performed by targeted haemagglutinin (HA) sequence analysis and/or whole genome sequencing for a subset of isolates (primer sequences available on request).
We describe here observations undertaken as part of routine national surveillance. These are carried out under National Health Service (NHS) Act 2006 (section 251), which provides statutory support for disclosure of such data by the NHS, and their processing by the Health Protection Agency (HPA) for communicable disease control [6].
Epidemiological findings
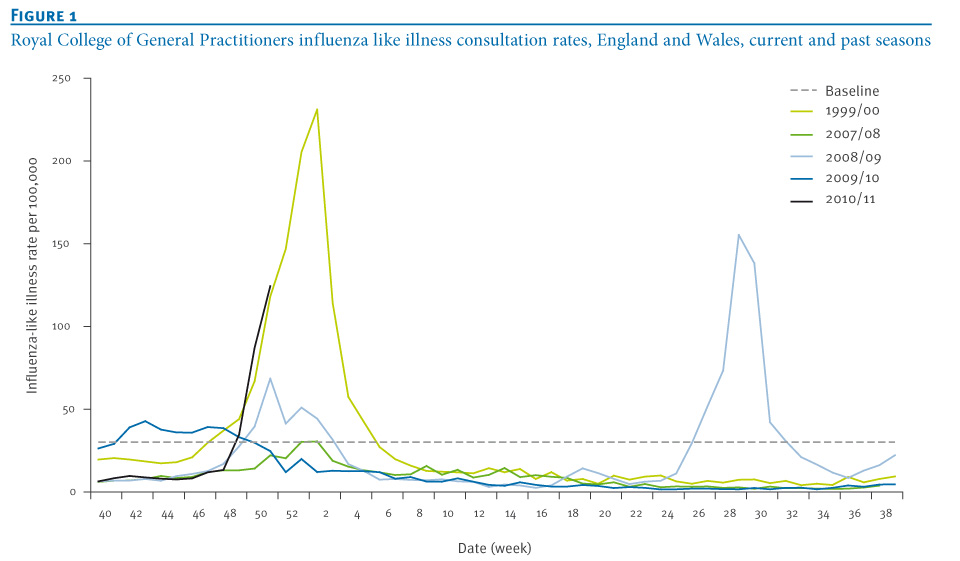
Early detections of influenza A(H1N1)2009 virus were first reported in weeks 40?42 from cases in the community. Indicators of clinical activity began to rise in week 47 crossing the traditional baseline threshold level indicating generalised influenza activity in the community in week 49, and have continued to increase up to week 52 (Figure 1).
Figure 1. Royal College of General Practitioners influenza like illness consultation rates, England and Wales, current and past seasons
Influenza A(H1N1)2009 viruses, followed by influenza B, have been the predominant influenza viruses circulating in the community in the period from October to the end of December 2010. Of 3,959 respiratory specimens reported to the English Data Mart system as taken in week 51, 1,711 (43.2%, increased from 38.9% in week 50) were positive for influenza, namely 1,402 influenza A(H1N1)2009, 41 not subtyped influenza A and 268 influenza B [7]. Since the beginning of the season, over 120 institutional outbreaks of respiratory illness have been reported, primarily from schools: 112 (93%) outbreaks from schools, four from care homes, two from hospitals, one from a military base, one from a nursery and two from prisons. Both influenza B and influenza A(H1N1)2009 have been detected in the few outbreaks that have been virologically investigated and confirmed: 22 outbreaks (44%) with influenza A(H1N1)2009 detected, 16 with influenza B, four with a mixture of influenza A(H1N1)2009 and influenza B, one with influenza A(H3N2) and seven with other respiratory viruses.
Admissions to hospital with severe illness have been reported. As of 30 December 2010, there were 738 patients with confirmed or suspected influenza in NHS critical care beds in England (42 cases under five years of age, 24 cases between five and 15 years, 586 cases between 16 and 64 years, and 86 cases 65 years and above) [8]. Thirty-nine deaths were reported between weeks 36 and 52 associated with confirmed influenza infection [7]. Four of the fatal cases were under five years of age, seven were 5-14 years of age, 27 cases were 15-64 years of age, and one fatal case was older than 64 years. The majority (36/39) of these deaths were associated with influenza A(H1N1)2009 infection, and three with influenza B infection. Underlying chronic conditions were reported in 23 of the 38 fatal cases for whom this information was available, with neurological disease such as cerebral palsy (n=9) and asthma (n=8) the most frequently reported underlying risk factors for vaccination [9]. Very few of the fatal cases (2/33) had received the 2010/11 trivalent influenza vaccine. A third of the cases (8/22) had not received antiviral therapy.
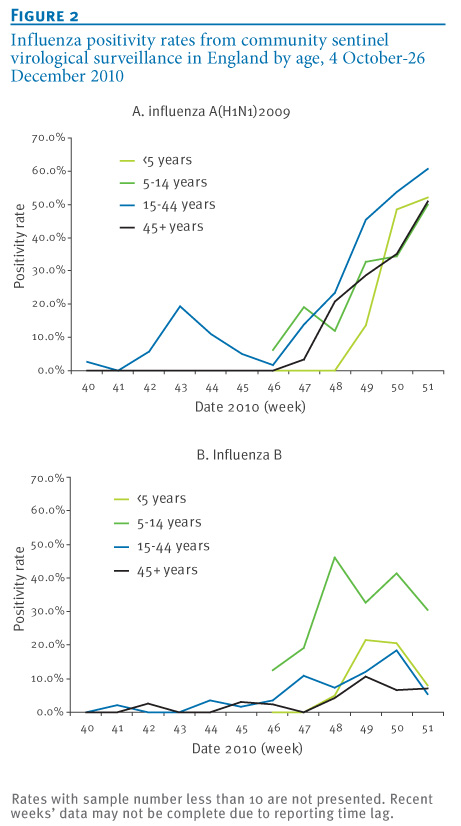
The proportion of samples from patients with influenza-like illness in sentinel general practitioner surveillance schemes in the community reported positive for influenza virus (A(H1N1)2009 or B) has risen rapidly to over 50% in week 49. The proportion of samples positive for influenza A(H1N1)2009 virus was highest in young adults (15-44 years), and for influenza B in children aged 5-14 years (Figure 2).
Figure 2. Influenza positivity rates from community sentinel virological surveillance in England by age, 4 October-26 December 2010

By week 50, the proportion of the population in England aged under 65 years in a risk group who had received the 2010/11 influenza vaccine was 43% [7].
Virological investigations
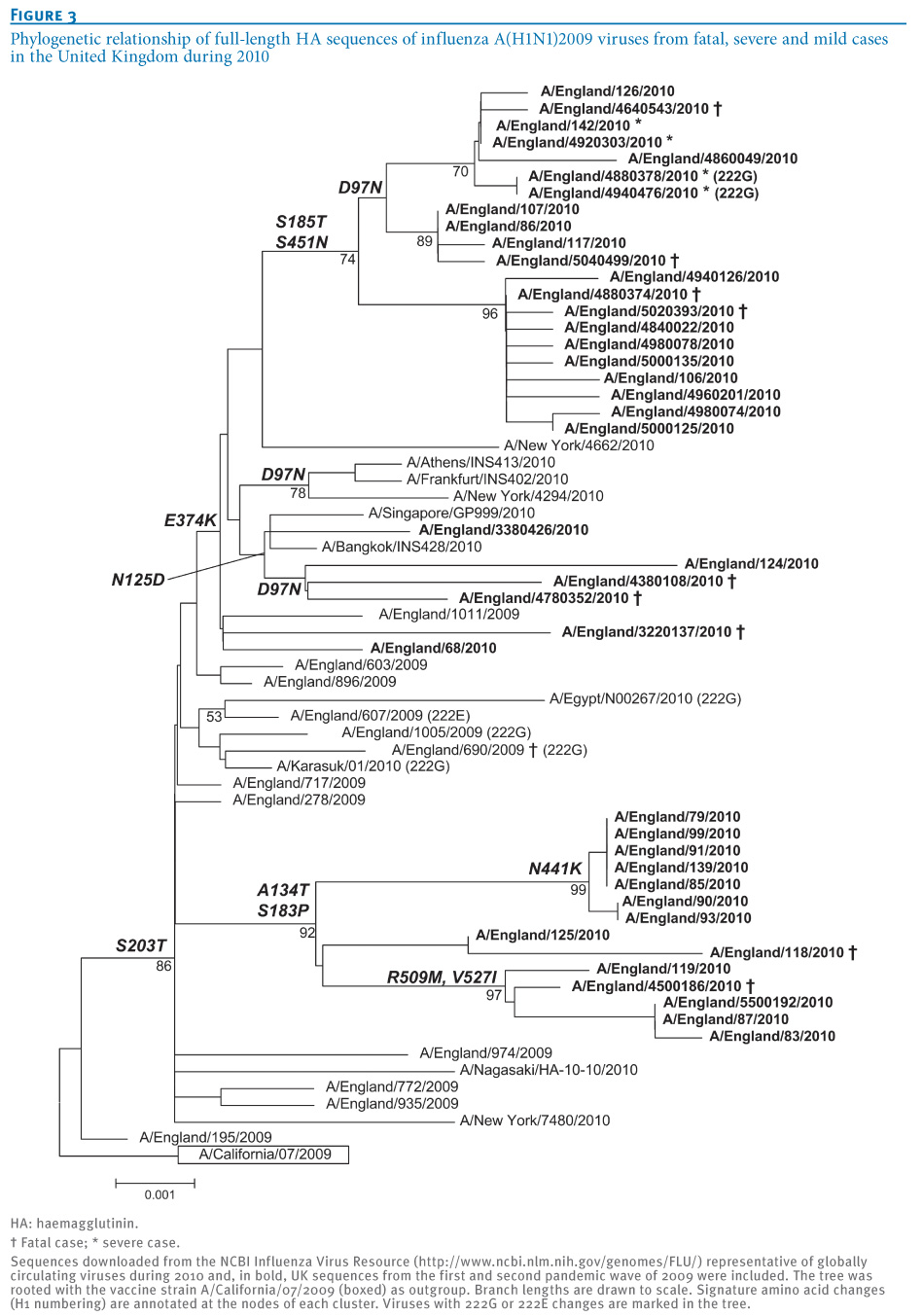
Influenza A(H1N1)2009 isolates characterised to date, in samples from the community, hospitalised patients and fatal cases, are antigenically homogeneous and similar to the A(H1N1)2009 virus included in the 2010/11 seasonal influenza vaccine, A/California/7/2009. Only minor genetic drift has been noted in influenza A(H1N1)2009 viruses circulating in 2010 compared with the earliest isolates in April 2009, and this observed genetic diversity has been consistent with expected patterns of virus evolution (Figure 3). Phylogenetic analysis shows that HA sequences from nine fatal and four severe cases in the UK in 2010 were interspersed with sequences from mild cases in 2010 from the UK and elsewhere. All UK 2010 viruses cluster in two main branches, characterised by either E374K with additional mutations in minor subclusters such as D97N, S185T, S451N and N125D, some of which have been recently described [10], or by A134T and S183P, with additional substitutions such as N441K, R509M and V527I. Almost all viruses from winter 2010 analysed to date from fatal and non-fatal cases had 222D in the HA gene (39/41).
Preliminary analyses from a limited number of whole genome sequences including some from fatal cases, indicate that these are consistent with observations from seasonal influenza and from the first and second waves of the recent pandemic: so far no unique mutations have been associated with severe or fatal cases of influenza A(H1N1)2009, but further comprehensive analysis is required.
Figure 3. Phylogenetic relationship of full-length HA sequences of influenza A(H1N1)2009 viruses from fatal, severe and mild cases in the United Kingdom during 2010

Between October and December 2010, antiviral resistance monitoring was undertaken on 156 community and 159 hospital isolates. Six cases of oseltamivir resistance associated with the H275Y mutation in the neuraminidase (NA) gene have been detected.Only one of these cases has had known exposure to oseltamivir, Two of them have been identified from community surveillance of uncomplicated infections, three cases have been detected before treatment in individuals hospitalised with underlying risk factors, and the sixth case has been detected after oseltamivir treatment in a hospitalised individual.
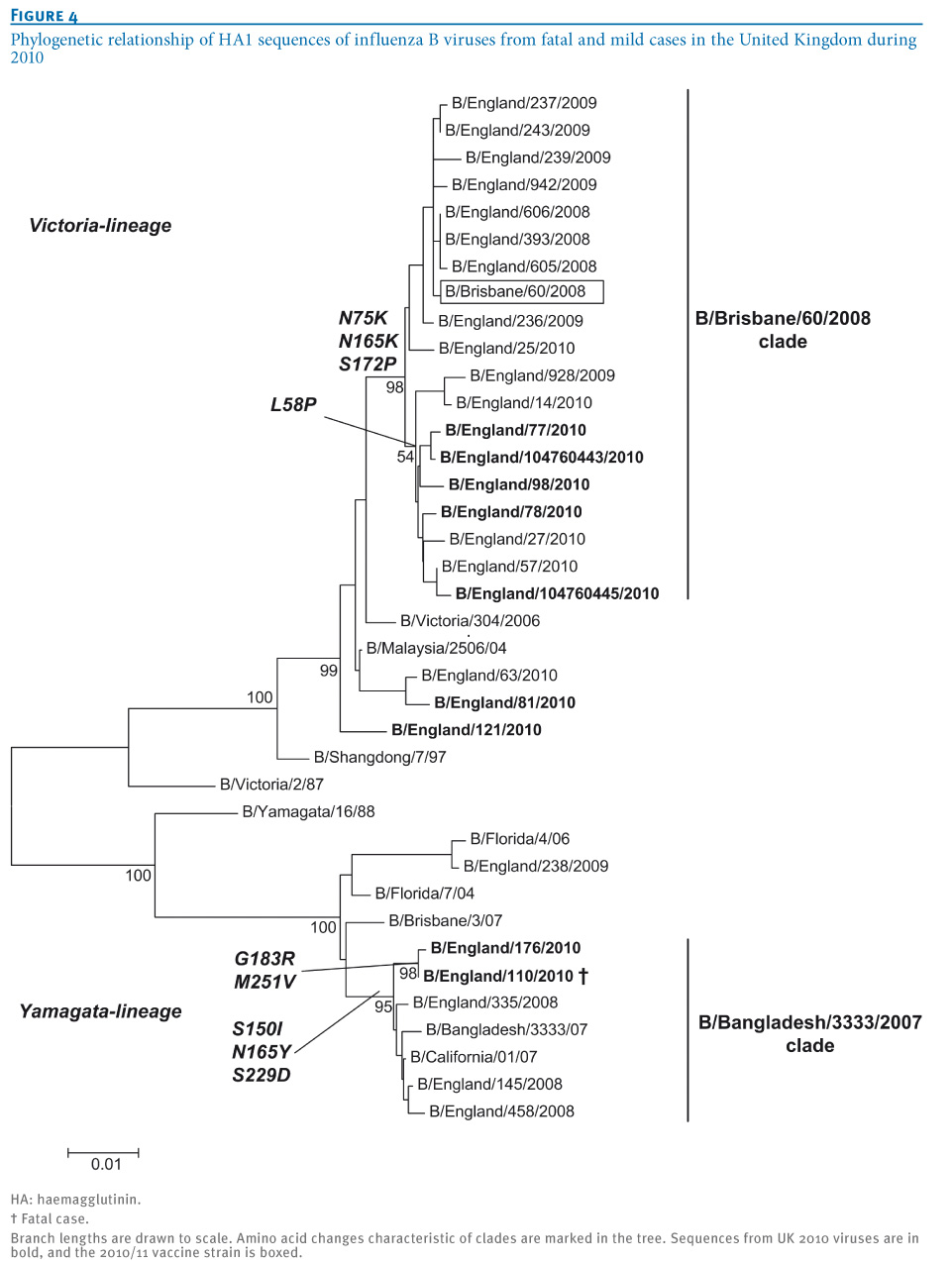
Over 98% of influenza B viruses isolated in the UK since week 40 in 2010 have been from the B/Victoria/2/87 lineage, with most showing good reactivity to antisera raised against reference viruses from this lineage. The HA sequences group within the genetic clade represented by the current vaccine strain, B/Brisbane/60/2008, characterised by amino acid substitutions L58P N75K, N165K and S172P (Figure 4). A separate small cluster of three viruses from the antigenically distinct B/Yamagata/16/88 lineage have also been detected in one region of England: one fatal case and two hospitalised cases. The three known fatal influenza B cases were distributed across both lineages. The HA segment of the influenza B/Yamagata lineage virus isolated from a fatal case in week 46 belonged to a clade represented by influenza B/Bangladesh/3333/2007, with amino acid substitutions S150I, N165Y and S229D relative to a previous vaccine strain, B/Florida/4/06. This HA sequence contained two additional substitutions, G183R and M251V, which had been sporadically detected in influenza B viruses isolated in several countries in 2009/10.
Figure 4. Phylogenetic relationship of HA1 sequences of influenza B viruses from fatal and mild cases in the United Kingdom during 2010

Antigenic characterisation of the few influenza A(H3N2) viruses detected since week 38 indicates that these viruses are closely related to A/Perth/16/2009, the influenza A(H3N2) 2010/11 vaccine strain.
Conclusions
Influenza virus circulation is underway in the UK and is contributing to seasonal winter pressures in the health system. The circulation of other winter viruses such as respiratory syncytial virus (RSV) and the particularly cold weather are also contributing. The virological picture is complex, with many strains of influenza virus circulating but no antigenic change in the influenza A(H1N1)2009 virus, and no immediately obvious genetic differences between viruses recovered from fatal cases and those causing mild illness. The picture of the illness associated with influenza A(H1N1)2009 infection is consistent with what was seen in the 2009 pandemic, with a similar demographic impact, particularly affecting children and young adults. Whilst young age groups have the least experience of influenza and are recognised as important in the transmission of influenza, it is also possible that propensity to consult a doctor is greatest in younger age groups. Although the remaining susceptibles in the age group under 15 year account for high rates of positivity in peak weeks in community samples (as is often the case during seasonal influenza), it is notable that overall, sustained high rates of positivity are most marked in the age group between 15 and 44 years. This is in contrast to earlier pandemic waves in 2009 when highest rates of positivity in the community were observed in the 5-14 year-olds. The age group of 15-44 year-olds is also clearly the major group contributing to hospital admissions and deaths. The increase in requirement for critical care in the current season reflects the impact of influenza A(H1N1)2009 illness in the remaining susceptible young adults (15-44 years) and risk groups in the population.
Most of those with severe illness, and those dying, have not previously been vaccinated against influenza and have not had the benefit of the early use of antiviral drugs. Countries in Europe yet to experience substantial influenza activity this winter may wish to take all reasonable measures to increase the uptake of seasonal influenza vaccine in those at high risk of the complications of influenza and to ensure that antiviral drugs are readily available for those who are either severely ill or at increased risk of severe illness from influenza.
Further analysis of the antigenic and genetic properties of all influenza viruses from hospitalised patients, outbreaks and community cases is ongoing.
Acknowledgements
The authors would like to acknowledge the contribution of the member laboratories of the Microbiology Services Division Laboratory Network, HPA, and participating RCGP practices, in submitting the clinical samples evaluated in this study. Technical and data support was provided by Richard Allan and the Respiratory Virus Unit, Microbiology Services: Colindale, Nichola Goddard, Microbiology Services: Colindale, Genomic Services Unit-AFGU, Department for Bioanalysis and Horizon Technologies, Microbiology Services: Colindale, and Respiratory Virus Department, Health Protection Services, Colindale, HPA. Thank you to John McCauley and Rod Daniels, WHO Collaborating Centre, UK, for useful discussions.
<hr> References
-
------
Eurosurveillance, Volume 16, Issue 1, 06 January 2011
Rapid communications
Virological analysis of fatal influenza cases in the United Kingdom during the early wave of influenza in winter 2010/11
J Ellis (
- Health Protection Agency, Centre for Infections, London, United Kingdom
<hr class="Centre_divider"> Citation style for this article: Ellis J, Galiano M, Pebody R, Lackenby A, Thompson C, Bermingham A, McLean E, Zhao H, Bolotin S, Dar O, Watson JM, Zambon M. Virological analysis of fatal influenza cases in the United Kingdom during the early wave of influenza in winter 2010/11. Euro Surveill. 2011;16(1):pii=19760. Available online: http://www.eurosurveillance.org/View...rticleId=19760
Date of submission: 31 December 2010 <hr class="Centre_divider">
<!-- Article start --> The 2010/11 winter influenza season is underway in the United Kingdom, with co-circulation of influenza A(H1N1)2009 (antigenically similar to the current 2010/11 vaccine strain), influenza B (mainly B/Victoria/2/87 lineage, similar to the 2010/11 vaccine strain) and a few sporadic influenza A(H3N2) viruses. Clinical influenza activity has been increasing. Severe illness, resulting in hospitalisation and deaths, has occurred in children and young adults and has predominantly been associated with influenza A(H1N1)2009, but also influenza B viruses.
<hr> Introduction
The onset of this winter season in the northern hemisphere is associated with more uncertainty than usual about which influenza viruses are likely to circulate and predominate, given the varying proportions of different virus strains circulating in the southern hemisphere between June and September 2010 [1]. Notably, influenza A(H3N2) predominated over influenza A(H1N1)2009 in several countries, e.g. South Africa and Chile. The second wave of the pandemic in the United Kingdom (UK) during the winter season of 2009/10 was almost exclusively associated with circulation of influenza A(H1N1)2009 [2]. Serological evaluation in the UK of population immunity to the pandemic strain after the second wave suggested that susceptibility was lowest in younger age groups (<15 years), with significant remaining susceptibility in the age group of 15?44 year-olds [3]. In view of the importance of children in the transmission of influenza A(H1N1)2009 [4], and the limited remaining susceptibility within this group, the probability of extensive morbidity in this age group associated with this strain in winter 2010/11 was considered unlikely in the absence of significant antigenic change in the pandemic virus. The extent, however, to which influenza A(H1N1)2009 would predominate over influenza A(H3N2) and cause illness in the remaining susceptible children and younger adults was unknown.
Investigations
Virological surveillance in the UK operates through hospital laboratories in secondary care and community-based schemes. Specimens containing influenza virus from community, hospitalised and fatal cases are forwarded to the UK National Influenza Centre for further characterisation. Samples are also received directly from sentinel primary care physicians participating in virological surveillance schemes in the community [5]. An antigenic typing profile is developed for each virus isolate and compared with influenza vaccine and reference strains. Genotypic and, where appropriate, phenotypic antiviral susceptibility analyses are performed on influenza-positive clinical material and/or virus isolates. Genetic characterisation is performed by targeted haemagglutinin (HA) sequence analysis and/or whole genome sequencing for a subset of isolates (primer sequences available on request).
We describe here observations undertaken as part of routine national surveillance. These are carried out under National Health Service (NHS) Act 2006 (section 251), which provides statutory support for disclosure of such data by the NHS, and their processing by the Health Protection Agency (HPA) for communicable disease control [6].
Epidemiological findings
Early detections of influenza A(H1N1)2009 virus were first reported in weeks 40?42 from cases in the community. Indicators of clinical activity began to rise in week 47 crossing the traditional baseline threshold level indicating generalised influenza activity in the community in week 49, and have continued to increase up to week 52 (Figure 1).
Figure 1. Royal College of General Practitioners influenza like illness consultation rates, England and Wales, current and past seasons
Influenza A(H1N1)2009 viruses, followed by influenza B, have been the predominant influenza viruses circulating in the community in the period from October to the end of December 2010. Of 3,959 respiratory specimens reported to the English Data Mart system as taken in week 51, 1,711 (43.2%, increased from 38.9% in week 50) were positive for influenza, namely 1,402 influenza A(H1N1)2009, 41 not subtyped influenza A and 268 influenza B [7]. Since the beginning of the season, over 120 institutional outbreaks of respiratory illness have been reported, primarily from schools: 112 (93%) outbreaks from schools, four from care homes, two from hospitals, one from a military base, one from a nursery and two from prisons. Both influenza B and influenza A(H1N1)2009 have been detected in the few outbreaks that have been virologically investigated and confirmed: 22 outbreaks (44%) with influenza A(H1N1)2009 detected, 16 with influenza B, four with a mixture of influenza A(H1N1)2009 and influenza B, one with influenza A(H3N2) and seven with other respiratory viruses.
Admissions to hospital with severe illness have been reported. As of 30 December 2010, there were 738 patients with confirmed or suspected influenza in NHS critical care beds in England (42 cases under five years of age, 24 cases between five and 15 years, 586 cases between 16 and 64 years, and 86 cases 65 years and above) [8]. Thirty-nine deaths were reported between weeks 36 and 52 associated with confirmed influenza infection [7]. Four of the fatal cases were under five years of age, seven were 5-14 years of age, 27 cases were 15-64 years of age, and one fatal case was older than 64 years. The majority (36/39) of these deaths were associated with influenza A(H1N1)2009 infection, and three with influenza B infection. Underlying chronic conditions were reported in 23 of the 38 fatal cases for whom this information was available, with neurological disease such as cerebral palsy (n=9) and asthma (n=8) the most frequently reported underlying risk factors for vaccination [9]. Very few of the fatal cases (2/33) had received the 2010/11 trivalent influenza vaccine. A third of the cases (8/22) had not received antiviral therapy.
The proportion of samples from patients with influenza-like illness in sentinel general practitioner surveillance schemes in the community reported positive for influenza virus (A(H1N1)2009 or B) has risen rapidly to over 50% in week 49. The proportion of samples positive for influenza A(H1N1)2009 virus was highest in young adults (15-44 years), and for influenza B in children aged 5-14 years (Figure 2).
Figure 2. Influenza positivity rates from community sentinel virological surveillance in England by age, 4 October-26 December 2010
By week 50, the proportion of the population in England aged under 65 years in a risk group who had received the 2010/11 influenza vaccine was 43% [7].
Virological investigations
Influenza A(H1N1)2009 isolates characterised to date, in samples from the community, hospitalised patients and fatal cases, are antigenically homogeneous and similar to the A(H1N1)2009 virus included in the 2010/11 seasonal influenza vaccine, A/California/7/2009. Only minor genetic drift has been noted in influenza A(H1N1)2009 viruses circulating in 2010 compared with the earliest isolates in April 2009, and this observed genetic diversity has been consistent with expected patterns of virus evolution (Figure 3). Phylogenetic analysis shows that HA sequences from nine fatal and four severe cases in the UK in 2010 were interspersed with sequences from mild cases in 2010 from the UK and elsewhere. All UK 2010 viruses cluster in two main branches, characterised by either E374K with additional mutations in minor subclusters such as D97N, S185T, S451N and N125D, some of which have been recently described [10], or by A134T and S183P, with additional substitutions such as N441K, R509M and V527I. Almost all viruses from winter 2010 analysed to date from fatal and non-fatal cases had 222D in the HA gene (39/41).
Preliminary analyses from a limited number of whole genome sequences including some from fatal cases, indicate that these are consistent with observations from seasonal influenza and from the first and second waves of the recent pandemic: so far no unique mutations have been associated with severe or fatal cases of influenza A(H1N1)2009, but further comprehensive analysis is required.
Figure 3. Phylogenetic relationship of full-length HA sequences of influenza A(H1N1)2009 viruses from fatal, severe and mild cases in the United Kingdom during 2010
Between October and December 2010, antiviral resistance monitoring was undertaken on 156 community and 159 hospital isolates. Six cases of oseltamivir resistance associated with the H275Y mutation in the neuraminidase (NA) gene have been detected.Only one of these cases has had known exposure to oseltamivir, Two of them have been identified from community surveillance of uncomplicated infections, three cases have been detected before treatment in individuals hospitalised with underlying risk factors, and the sixth case has been detected after oseltamivir treatment in a hospitalised individual.
Over 98% of influenza B viruses isolated in the UK since week 40 in 2010 have been from the B/Victoria/2/87 lineage, with most showing good reactivity to antisera raised against reference viruses from this lineage. The HA sequences group within the genetic clade represented by the current vaccine strain, B/Brisbane/60/2008, characterised by amino acid substitutions L58P N75K, N165K and S172P (Figure 4). A separate small cluster of three viruses from the antigenically distinct B/Yamagata/16/88 lineage have also been detected in one region of England: one fatal case and two hospitalised cases. The three known fatal influenza B cases were distributed across both lineages. The HA segment of the influenza B/Yamagata lineage virus isolated from a fatal case in week 46 belonged to a clade represented by influenza B/Bangladesh/3333/2007, with amino acid substitutions S150I, N165Y and S229D relative to a previous vaccine strain, B/Florida/4/06. This HA sequence contained two additional substitutions, G183R and M251V, which had been sporadically detected in influenza B viruses isolated in several countries in 2009/10.
Figure 4. Phylogenetic relationship of HA1 sequences of influenza B viruses from fatal and mild cases in the United Kingdom during 2010
Antigenic characterisation of the few influenza A(H3N2) viruses detected since week 38 indicates that these viruses are closely related to A/Perth/16/2009, the influenza A(H3N2) 2010/11 vaccine strain.
Conclusions
Influenza virus circulation is underway in the UK and is contributing to seasonal winter pressures in the health system. The circulation of other winter viruses such as respiratory syncytial virus (RSV) and the particularly cold weather are also contributing. The virological picture is complex, with many strains of influenza virus circulating but no antigenic change in the influenza A(H1N1)2009 virus, and no immediately obvious genetic differences between viruses recovered from fatal cases and those causing mild illness. The picture of the illness associated with influenza A(H1N1)2009 infection is consistent with what was seen in the 2009 pandemic, with a similar demographic impact, particularly affecting children and young adults. Whilst young age groups have the least experience of influenza and are recognised as important in the transmission of influenza, it is also possible that propensity to consult a doctor is greatest in younger age groups. Although the remaining susceptibles in the age group under 15 year account for high rates of positivity in peak weeks in community samples (as is often the case during seasonal influenza), it is notable that overall, sustained high rates of positivity are most marked in the age group between 15 and 44 years. This is in contrast to earlier pandemic waves in 2009 when highest rates of positivity in the community were observed in the 5-14 year-olds. The age group of 15-44 year-olds is also clearly the major group contributing to hospital admissions and deaths. The increase in requirement for critical care in the current season reflects the impact of influenza A(H1N1)2009 illness in the remaining susceptible young adults (15-44 years) and risk groups in the population.
Most of those with severe illness, and those dying, have not previously been vaccinated against influenza and have not had the benefit of the early use of antiviral drugs. Countries in Europe yet to experience substantial influenza activity this winter may wish to take all reasonable measures to increase the uptake of seasonal influenza vaccine in those at high risk of the complications of influenza and to ensure that antiviral drugs are readily available for those who are either severely ill or at increased risk of severe illness from influenza.
Further analysis of the antigenic and genetic properties of all influenza viruses from hospitalised patients, outbreaks and community cases is ongoing.
Acknowledgements
The authors would like to acknowledge the contribution of the member laboratories of the Microbiology Services Division Laboratory Network, HPA, and participating RCGP practices, in submitting the clinical samples evaluated in this study. Technical and data support was provided by Richard Allan and the Respiratory Virus Unit, Microbiology Services: Colindale, Nichola Goddard, Microbiology Services: Colindale, Genomic Services Unit-AFGU, Department for Bioanalysis and Horizon Technologies, Microbiology Services: Colindale, and Respiratory Virus Department, Health Protection Services, Colindale, HPA. Thank you to John McCauley and Rod Daniels, WHO Collaborating Centre, UK, for useful discussions.
<hr> References
- Influenza Update 117. Geneva: World Health Organization; 24 September 2010. Available from: http://www.who.int/csr/disease/influ.../en/index.html
- Epidemiological report of pandemic (H1N1) 2009 in the UK. London: Health Protection Agency; October 2010. Available from: http://www.hpa.org.uk/Publications/I...cH1N12009inUK/
- Hardelid P, Andrews NJ, Hoschler K, Stanford E, Baguelin M, Waight PA, et al. Assessment of baseline age-specific antibody prevalence and incidence of infection to novel influenza AH1N1 2009. Health Technology Assessment. 2010; 14(55): 115?92.
- Ghani AC, Baguelin M, Griffin J, Flasche S, Pebody R, van Hoek AJ, et al. The early transmission dynamics of H1N1 pdm influenza in the United Kingdom. PLoS Curr. 2009 Nov 16;1:RRN1130.
- Fleming DM, Chakraverty P, Sadler C, Litton P. Combined clinical and virological surveillance of influenza in winters of 1992 and 1993-4. BMJ. 1995:311(7000):290-1.
- The National Health Service Act 2006, The National Health Service (Wales) Act 2006 and The National Health Service (Consequential Provisions) Act 2006. London: Department of Health; 21 December 2010. Available from: http://www.dh.gov.uk/en/Publications...ills/DH_064103
- HPA Weekly National Influenza Report; Summary of UK surveillance of influenza and other seasonal respiratory illnesses? Week 52. London: Health Protection Agency; 30 December 2010. Available from: http://www.hpa.org.uk/web/HPAwebFile.../1287147913387
- Winterwatch. Winter health data. London: Department of Health; 30 December 2010. Available from: http://winterwatch.dh.gov.uk/winter-...december-2010/
- Influenza. In: Immunisation against infection disease ? ?The Green Book?. London: Department of Health; 24 December 2010. Available from: http://www.dh.gov.uk/prod_consum_dh/.../dh_123162.pdf
- Barr IG, Cui L, Komadina N, Lee RT, Lin RT, Deng Y, et al. A new pandemic influenza A(H1N1) genetic variant predominated in the winter 2010 influenza season in Australia, New Zealand and Singapore. Euro Surveill. 2010;15(42):pii=19692. Available from: http://www.eurosurveillance.org/View...rticleId=19692
-
------