 Tweet
Tweet
Severe hospitalised 2009 pandemic influenza A(H1N1) cases in France, 1 July-15 November 2009 (Euro Surveill., edited)
Eurosurveillance, Volume 15, Issue 2, 14 January 2010
Surveillance and outbreak reports
Severe hospitalised 2009 pandemic influenza A(H1N1) cases in France, 1 July-15 November 2009
C Fuhrman ( )<sup>1</sup>, I Bonmarin<sup>1</sup>, A C Paty<sup>1</sup>, N Duport<sup>1</sup>, E Chiron<sup>1</sup>, E Lucas<sup>1</sup>, D Bitar<sup>1</sup>, A Mailles<sup>1</sup>, M Herida<sup>1</sup>, S Vaux<sup>1</sup>, D L?vy-Bruhl<sup>1</sup>
)<sup>1</sup>, I Bonmarin<sup>1</sup>, A C Paty<sup>1</sup>, N Duport<sup>1</sup>, E Chiron<sup>1</sup>, E Lucas<sup>1</sup>, D Bitar<sup>1</sup>, A Mailles<sup>1</sup>, M Herida<sup>1</sup>, S Vaux<sup>1</sup>, D L?vy-Bruhl<sup>1</sup>
<hr>
Citation style for this article: Fuhrman C, Bonmarin I, Paty AC, Duport N, Chiron E, Lucas E, Bitar D, Mailles A, Herida M, Vaux S, L?vy-Bruhl D. Severe hospitalised 2009 pandemic influenza A(H1N1) cases in France, 1 July-15 November 2009. Euro Surveill. 2010;15(2):pii=19463. Available online: http://www.eurosurveillance.org/View...rticleId=19463
Date of submission: 14 December 2009
<hr>
From 1 July 2009 to 15 November 2009, 244 patients with 2009 pandemic influenza A(H1N1) were admitted to intensive care units (ICU) and were compared with 514 cases hospitalised in medical wards in France until 2 November 2009. Detailed case-based epidemiological information and outcomes were gathered for all hospitalised cases. Infants and pregnant women are overrepresented among cases admitted to ICU with seven per cent for both groups respectively, and twenty per cent of ICU cases did not belong to a risk group. Chronic respiratory disease was the most common risk factor among cases but obesity (body mass index ≥ 30 Kg/m<sup>2</sup>), chronic cardiac disease and immunosuppression were risk factors associated with severe illness after adjustment for age and for other co-morbidities.
<hr>
Introduction
On 1 May 2009, the first two cases of 2009 pandemic influenza A(H1N1) were identified in France [1]. At this time, hospitalisation of all cases was required, irrespective of their clinical presentation. After the virus had spread more widely and community transmission had increased, systematic hospitalisation was discontinued on 1 July. At the same time, a national hospital-based surveillance system of hospitalised 2009 pandemic influenza cases was set-up by the National Institute for Public Health Surveillance (Institut de veille sanitaire, InVS). The surveillance of hospitalised pandemic influenza cases was restricted to patients with severe disease on 2 November when there had been a sharp rise in the total number of cases requiring hospital admission.
In this paper we describe the characteristics and outcome of severe cases of pandemic influenza hospitalised in metropolitan France between 1 July and 15 November, 2009 and identify risk factors for severe outcome and death, respectively.
Methods
In France, a nationwide hospital-based surveillance system was implemented on 1 July 2009. Clinicians were requested to report to InVS all hospitalised cases of pandemic influenza through a standardised notification form available on the InVS website. Patients to be notified included (i) those with a positive RT-PCR performed on a nasal swab, (ii) patients with a severe clinical influenza, likely to be caused by 2009 pandemic influenza virus according to the clinician, even in the absence of laboratory confirmation, and (iii) patients with an epidemiological link with a confirmed case of pandemic influenza. Two levels of severity of disease were defined: non-severe (hospitalised in medical wards for at least 24 hours) and severe (admitted to ICU or death while hospitalised).
Follow-up data for cases were collected weekly by telephone contact between InVS staff (epidemiologists or physicians) and physicians in charge of the patient until discharge or death. At discharge, clinicians were invited to return a second notification form also available on the InVS website. The forms received were cross-checked with individual positive PCR results coming from the network of all laboratories performing the RT-PCR for the 2009 pandemic influenza virus.
Descriptive statistics included frequency analysis (percentages) for categorical variables and median and interquartile ranges (IQR) for continuous variables. The differences in characteristics according to outcomes were tested using chi-squared test for categorical variables and Mann-Whitney rank sum test for continuous variables. A p-value under 0.05 was considered statistically significant. Two types of comparison were made. First, the clinical characteristics of patients with severe disease were compared with those of patients admitted to medical wards until 2 November 2009. Second, clinical characteristics of surviving severe cases discharged before 15 November, were compared with those of fatal cases. Odds ratios (OR), including 95% confidence intervals (CI), were calculated through multivariate logistic regression analysis. We included in the analysis the presence or absence of each of the following underlying medical conditions/ potential risk factors: chronic respiratory disease, pregnancy, diabetes, obesity (body mass index ≥ 30 Kg/m<sup>2</sup>), immunosupression and chronic cardiac disease as categorical variables. The analysis was performed with Stata V9.
Results
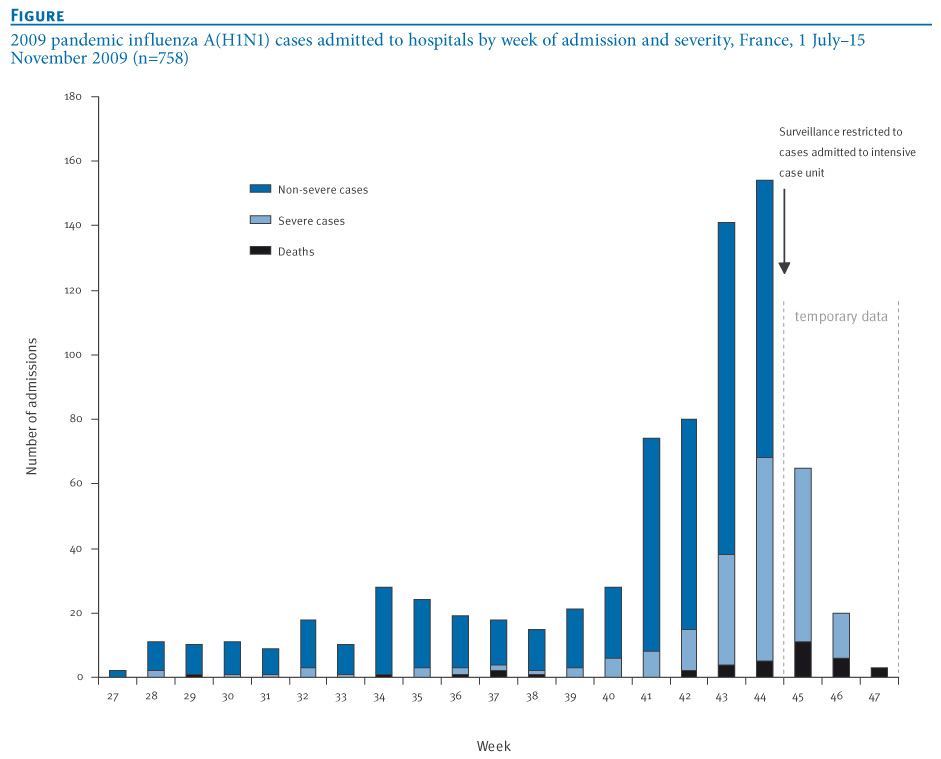
From 1 July to 15 November and 2 November 2009 respectively, 244 severe cases of 2009 pandemic influenza and 514 cases hospitalised in medical wards were reported to InVS. The number of hospitalisations increased sharply from week 41 (Figure 1). Almost all cases (98%) were laboratory confirmed as 2009 pandemic influenza A(H1N1), the 2% non-laboratory confirmed cases were patients with clinical influenza and/or patients with an epidemiological link with a confirmed case.
Figure. 2009 pandemic influenza A(H1N1) cases admitted to hospitals by week of admission and severity, France, 1 July?15 November 2009 (n=758)
Clinical characteristics
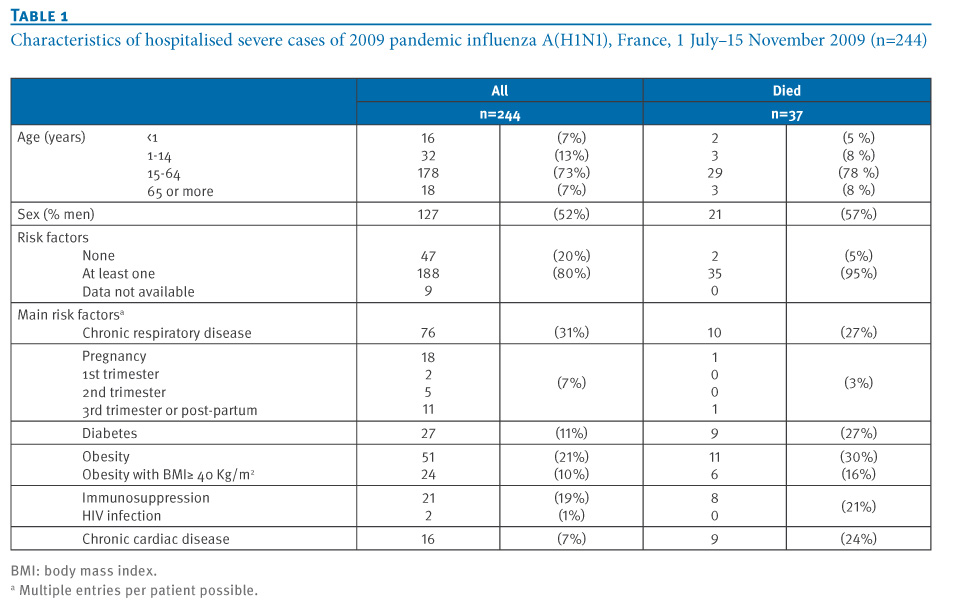
Among the 244 severe cases, 48 (20%) were children under 15 years of age, the male/female ratio was 1.1 (Table 1). The age-specific incidence of admission to ICU was highest among infants (children under one year of age, 2.03 cases per 100,000 of the age group and lowest among those 65 years of age or older (0.18 cases/100,000 of the age group).
Underlying conditions were present in 188 (80%) patients. This proportion was 67% among children. Chronic respiratory diseases were the most common underlying condition, both in adults and children. Of the 117 women, 18 were either pregnant, mainly in the second (n=5) and third trimester, or had recently delivered (i.e. within a week) (n=11). Among these 18 women, 61% had an underlying medical condition.
Table 1. Characteristics of hospitalised severe cases of 2009 pandemic influenza A(H1N1), France, 1 July?15 November 2009 (n=244)

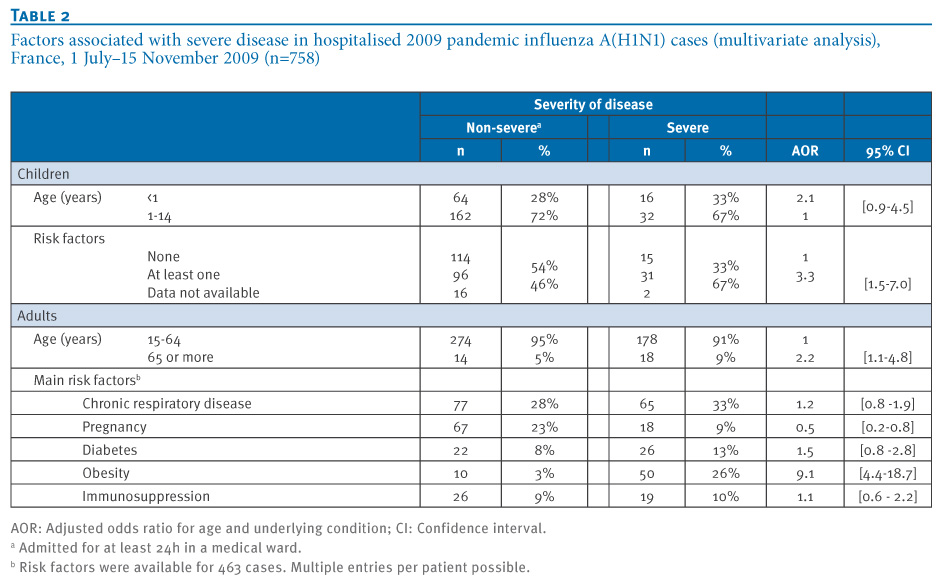
Compared with non-severe hospitalised paediatric cases, the risk of severe disease was significantly higher for children with an underlying condition (age-adjusted OR: 3.3); the excess risk associated with younger age (<1 year) however, did not reach statistical significance (Table 2).
Table 2. Factors associated with severe disease in hospitalised 2009 pandemic influenza A(H1N1) cases (multivariate analysis), France, 1 July?15 November 2009 (n=758)

In the multivariate analysis, increasing age and obesity were significantly associated with severe disease when compared with non-severe hospitalised adult cases (adjusted OR 2.2; 95% CI 1.1 to 4.8) for age 65 years or more and 9.1 (95% CI 4.4 to 18.7) for obesity) (Table 2).
Pregnancy was more prevalent among female cases aged 15-45 years admitted to medical wards than among those in this age group admitted to ICU (50% and 31% respectively, p=0.02). Among pregnant women, having an underlying condition was significantly associated with severe disease (age-adjusted OR: 8.4; 95% CI 2.5 to 28.6).
Interval from symptom to admission and treatment
The interval from onset of symptoms to admission was available for 216 severe cases and 427 non-severe cases. The median interval was 2.0 days (range 0-31) for severe cases and significantly longer than for cases without severity criteria: 1.2 days (range 0-13) (p<0.001). Data about antiviral therapy were available for 153 severe and 306 non-severe cases; 93% of severe cases had received antiviral therapy (oseltamivir) versus 81% of non-severe cases. Information for the interval from onset of symptoms to antiviral treatment initiation was available for 322 patients (207 non-severe and 115 severe). This interval was ≤2 days for 153 (74%) non-severe cases and for 45 (39%) cases patients (p<0.001). Similar results were obtained when the analysis was restricted to cases with underlying disease: 100 (72%) of the non-severe cases and 38 (41%) of severe cases had received early antiviral therapy (p<0.001).
Outcome
Of the 244 severe cases, 147 (60%) required ventilator support, 60 (25%) had an acute respiratory distress syndrome (ARDS) and 21 (9%) required extracorporeal membrane oxygenation (ECMO). At the time of analysis, 143 patients had been discharged from the ICU, and 37 (15%) had died. The median length of stay in the ICU was five days (IQR 3-8). The median age of patients who died was 42 years (range 8 months-71 years) and the median time from hospital admission to death was four days (range 0-74). Among the five children who died, three were one year old or under, one was six and one was 14 years old and all of them had at least one underlying condition. Among the 32 adults who died, 30 (94%) had at least one underlying condition (Table 1). A pregnant woman with underlying condition died.
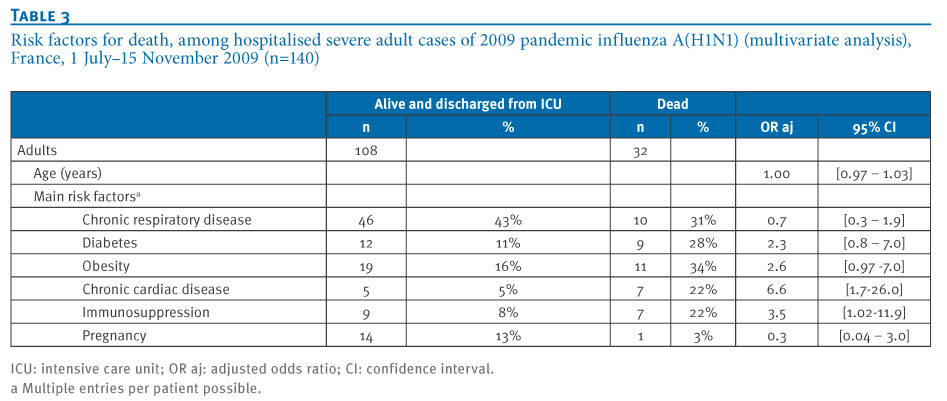
Chronic cardiac disease and immunosuppression were associated with fatal outcome but this was not the case for chronic respiratory diseases. Obesity had an OR point estimate of 2.6 but was not statistically significant (Table 3).
Table 3. Risk factors for death, among hospitalised severe adult 2009 pandemic influenza A(H1N1) cases (multivariate analysis), France, 1 July?15 November 2009 (n=140)

Discussion
This series of hospitalised patients with 2009 pandemic influenza confirms that the 2009 pandemic virus can induce severe illness among children and adults, even for those with no underlying medical conditions. The epidemic started almost two months before the usual influenza season in France. No co-circulation of other influenza viruses was identified through the enhanced virological surveillance during the period of data collection.
In our series, the highest ICU admission rate was found in infants and the lowest in the elderly. Being 65 years old or more seems, to be a risk factor for severe disease when hospitalised, but not for death, after adjustment for the presence of co-morbidities. Our results are coherent with other reports on 2009 pandemic influenza. In Australia and New Zealand, the rate of admission to ICU was low in the elderly but the risk of death increased with age [2]. In the analysis of Mexican data, confirmed cases aged 70 years or more, had the lowest mortality rate but the highest death to hospital admission ratio [3]. We did not identify an association for cases between death and being more than 65 years old. This could be explained by the fact that our analysis was adjusted to the presence of co-morbidity. It may also be due to the limited sample size of our series.
The underlying conditions leading to more severe illness we found are those reported in the literature. Chronic respiratory illness is the most prevalent in our case series, as described also by Jain et al. [4], but it is not associated with a higher risk of more severe disease or death among hospitalised cases. In contrast, obesity is clearly a risk factor for severe disease and probably for death as was reported in the literature [2,4,5]. Obesity is a risk factor for severe viral pneumonia [6] while severity connected to chronic respiratory disease is related to the exacerbation of the disease, and is usually responsive to bronchodilatator treatment [7]. Pregnancy, especially at the end of the gestation, is overrepresented among the patients hospitalised and accounts for 7% of admissions to ICU whereas pregnancy (estimated from the number of live birth in 2008 and the number of abortions in France) represents around 1% of the general population. Our finding confirms that pregnancy should be considered as a risk factor for complications from 2009 pandemic influenza [8]. A similar conclusion stands for infants, also accounting for 7% of admissions to ICU.
The interval from the onset of symptoms to admission was longer for severe cases than for non-severe cases. Furthermore, antiviral treatment was initiated less than 48 hours after the onset of symptoms for 74% of non-severe hospitalised cases and 39% for severe cases. As already suggested by data from the United States, it is possible that delayed initiation of antiviral therapy may have contributed to increased severity of illness [4,9]. Communication to patients and physicians should be strengthened on the need for rapid initiation of treatment, whenever indicated.
Of the 244 patients with severe disease, 60 % required ventilator support, 25% had an acute respiratory distress syndrome (ARDS) and 9% required extracorporeal membrane oxygenation (ECMO). Theses results are also consistent with previously published reports [2,4].
Our study has several limitations. Although our surveillance was implemented in the context of public health emergency some cases may have not been reported to InVS. However, several factors are in favour of only few cases having been missed. Firstly, only a few additional cases were identified after cross-checking with data from laboratories. Secondly, cases considered by clinicians as likely to be due to 2009 pandemic influenza, even in the absence of laboratory confirmation, were included in the definition of cases to be notified. Thirdly, regular phone calls with physicians of ICU wards were made by InVS staff in order to complete missing information on received forms and ask for cases not notified. Last but not least, the hospital surveillance is strongly supported by various ICU medical practitioners? societies.
To assess risk factors for severe clinical presentation we used 2009 pandemic influenza cases admitted to medical wards as a control group. This choice of controls may have lead to an underestimation of odds ratios because for some specific population groups potentially more prone to complications such as pregnant women and children, individuals may have been hospitalised as a precautionary measure even in the absence of severe disease. This could explain our finding of a higher proportion of non-severely ill pregnant women hospitalised in medical wards compared to those admitted to ICU.
Our study confirms the role of the underlying conditions as risk factors for severe disease and strengthens the need for a rapid start of antiviral therapy, especially for patients with underlying conditions. Furthermore, it confirms the French national strategy which recommends priority vaccination of pregnant women, close contacts of infants and patients of any age with co-morbidities known to increase the risk of severe influenza.
Our analysis will be renewed when a larger series of cases will be available: as of 2 December, 511 severe cases have been identified with 74 deaths and the epidemic does not seem to have reached its peak yet.
Acknowledgements
We thank all clinicians and the following medical societies: Soci?t? de R?animation de Langue Fran?aise (SRLF), Groupe Francophone de R?animation et Urgences P?diatriques (GFRUP), Soci?t? Fran?aise d'Anesth?sie et de R?animation (SFAR) who were involved in the collection and contribution of clinical data and all laboratories who contributed with RT-PCR results. We also thank all colleagues at InVS who were directly or indirectly involved in the influenza surveillance for their support, especially the regional units of the InVS (CIRES) and we thank Christine Saura and Jean-Claude Desenclos for their advice and support.
<hr>
References
-
------
Eurosurveillance, Volume 15, Issue 2, 14 January 2010
Surveillance and outbreak reports
Severe hospitalised 2009 pandemic influenza A(H1N1) cases in France, 1 July-15 November 2009
C Fuhrman (
- Institut de veille sanitaire, Saint-Maurice, France
<hr>
Citation style for this article: Fuhrman C, Bonmarin I, Paty AC, Duport N, Chiron E, Lucas E, Bitar D, Mailles A, Herida M, Vaux S, L?vy-Bruhl D. Severe hospitalised 2009 pandemic influenza A(H1N1) cases in France, 1 July-15 November 2009. Euro Surveill. 2010;15(2):pii=19463. Available online: http://www.eurosurveillance.org/View...rticleId=19463
Date of submission: 14 December 2009
<hr>
From 1 July 2009 to 15 November 2009, 244 patients with 2009 pandemic influenza A(H1N1) were admitted to intensive care units (ICU) and were compared with 514 cases hospitalised in medical wards in France until 2 November 2009. Detailed case-based epidemiological information and outcomes were gathered for all hospitalised cases. Infants and pregnant women are overrepresented among cases admitted to ICU with seven per cent for both groups respectively, and twenty per cent of ICU cases did not belong to a risk group. Chronic respiratory disease was the most common risk factor among cases but obesity (body mass index ≥ 30 Kg/m<sup>2</sup>), chronic cardiac disease and immunosuppression were risk factors associated with severe illness after adjustment for age and for other co-morbidities.
<hr>
Introduction
On 1 May 2009, the first two cases of 2009 pandemic influenza A(H1N1) were identified in France [1]. At this time, hospitalisation of all cases was required, irrespective of their clinical presentation. After the virus had spread more widely and community transmission had increased, systematic hospitalisation was discontinued on 1 July. At the same time, a national hospital-based surveillance system of hospitalised 2009 pandemic influenza cases was set-up by the National Institute for Public Health Surveillance (Institut de veille sanitaire, InVS). The surveillance of hospitalised pandemic influenza cases was restricted to patients with severe disease on 2 November when there had been a sharp rise in the total number of cases requiring hospital admission.
In this paper we describe the characteristics and outcome of severe cases of pandemic influenza hospitalised in metropolitan France between 1 July and 15 November, 2009 and identify risk factors for severe outcome and death, respectively.
Methods
In France, a nationwide hospital-based surveillance system was implemented on 1 July 2009. Clinicians were requested to report to InVS all hospitalised cases of pandemic influenza through a standardised notification form available on the InVS website. Patients to be notified included (i) those with a positive RT-PCR performed on a nasal swab, (ii) patients with a severe clinical influenza, likely to be caused by 2009 pandemic influenza virus according to the clinician, even in the absence of laboratory confirmation, and (iii) patients with an epidemiological link with a confirmed case of pandemic influenza. Two levels of severity of disease were defined: non-severe (hospitalised in medical wards for at least 24 hours) and severe (admitted to ICU or death while hospitalised).
Follow-up data for cases were collected weekly by telephone contact between InVS staff (epidemiologists or physicians) and physicians in charge of the patient until discharge or death. At discharge, clinicians were invited to return a second notification form also available on the InVS website. The forms received were cross-checked with individual positive PCR results coming from the network of all laboratories performing the RT-PCR for the 2009 pandemic influenza virus.
Descriptive statistics included frequency analysis (percentages) for categorical variables and median and interquartile ranges (IQR) for continuous variables. The differences in characteristics according to outcomes were tested using chi-squared test for categorical variables and Mann-Whitney rank sum test for continuous variables. A p-value under 0.05 was considered statistically significant. Two types of comparison were made. First, the clinical characteristics of patients with severe disease were compared with those of patients admitted to medical wards until 2 November 2009. Second, clinical characteristics of surviving severe cases discharged before 15 November, were compared with those of fatal cases. Odds ratios (OR), including 95% confidence intervals (CI), were calculated through multivariate logistic regression analysis. We included in the analysis the presence or absence of each of the following underlying medical conditions/ potential risk factors: chronic respiratory disease, pregnancy, diabetes, obesity (body mass index ≥ 30 Kg/m<sup>2</sup>), immunosupression and chronic cardiac disease as categorical variables. The analysis was performed with Stata V9.
Results
From 1 July to 15 November and 2 November 2009 respectively, 244 severe cases of 2009 pandemic influenza and 514 cases hospitalised in medical wards were reported to InVS. The number of hospitalisations increased sharply from week 41 (Figure 1). Almost all cases (98%) were laboratory confirmed as 2009 pandemic influenza A(H1N1), the 2% non-laboratory confirmed cases were patients with clinical influenza and/or patients with an epidemiological link with a confirmed case.
Figure. 2009 pandemic influenza A(H1N1) cases admitted to hospitals by week of admission and severity, France, 1 July?15 November 2009 (n=758)
Clinical characteristics
Among the 244 severe cases, 48 (20%) were children under 15 years of age, the male/female ratio was 1.1 (Table 1). The age-specific incidence of admission to ICU was highest among infants (children under one year of age, 2.03 cases per 100,000 of the age group and lowest among those 65 years of age or older (0.18 cases/100,000 of the age group).
Underlying conditions were present in 188 (80%) patients. This proportion was 67% among children. Chronic respiratory diseases were the most common underlying condition, both in adults and children. Of the 117 women, 18 were either pregnant, mainly in the second (n=5) and third trimester, or had recently delivered (i.e. within a week) (n=11). Among these 18 women, 61% had an underlying medical condition.
Table 1. Characteristics of hospitalised severe cases of 2009 pandemic influenza A(H1N1), France, 1 July?15 November 2009 (n=244)
Compared with non-severe hospitalised paediatric cases, the risk of severe disease was significantly higher for children with an underlying condition (age-adjusted OR: 3.3); the excess risk associated with younger age (<1 year) however, did not reach statistical significance (Table 2).
Table 2. Factors associated with severe disease in hospitalised 2009 pandemic influenza A(H1N1) cases (multivariate analysis), France, 1 July?15 November 2009 (n=758)
In the multivariate analysis, increasing age and obesity were significantly associated with severe disease when compared with non-severe hospitalised adult cases (adjusted OR 2.2; 95% CI 1.1 to 4.8) for age 65 years or more and 9.1 (95% CI 4.4 to 18.7) for obesity) (Table 2).
Pregnancy was more prevalent among female cases aged 15-45 years admitted to medical wards than among those in this age group admitted to ICU (50% and 31% respectively, p=0.02). Among pregnant women, having an underlying condition was significantly associated with severe disease (age-adjusted OR: 8.4; 95% CI 2.5 to 28.6).
Interval from symptom to admission and treatment
The interval from onset of symptoms to admission was available for 216 severe cases and 427 non-severe cases. The median interval was 2.0 days (range 0-31) for severe cases and significantly longer than for cases without severity criteria: 1.2 days (range 0-13) (p<0.001). Data about antiviral therapy were available for 153 severe and 306 non-severe cases; 93% of severe cases had received antiviral therapy (oseltamivir) versus 81% of non-severe cases. Information for the interval from onset of symptoms to antiviral treatment initiation was available for 322 patients (207 non-severe and 115 severe). This interval was ≤2 days for 153 (74%) non-severe cases and for 45 (39%) cases patients (p<0.001). Similar results were obtained when the analysis was restricted to cases with underlying disease: 100 (72%) of the non-severe cases and 38 (41%) of severe cases had received early antiviral therapy (p<0.001).
Outcome
Of the 244 severe cases, 147 (60%) required ventilator support, 60 (25%) had an acute respiratory distress syndrome (ARDS) and 21 (9%) required extracorporeal membrane oxygenation (ECMO). At the time of analysis, 143 patients had been discharged from the ICU, and 37 (15%) had died. The median length of stay in the ICU was five days (IQR 3-8). The median age of patients who died was 42 years (range 8 months-71 years) and the median time from hospital admission to death was four days (range 0-74). Among the five children who died, three were one year old or under, one was six and one was 14 years old and all of them had at least one underlying condition. Among the 32 adults who died, 30 (94%) had at least one underlying condition (Table 1). A pregnant woman with underlying condition died.
Chronic cardiac disease and immunosuppression were associated with fatal outcome but this was not the case for chronic respiratory diseases. Obesity had an OR point estimate of 2.6 but was not statistically significant (Table 3).
Table 3. Risk factors for death, among hospitalised severe adult 2009 pandemic influenza A(H1N1) cases (multivariate analysis), France, 1 July?15 November 2009 (n=140)
Discussion
This series of hospitalised patients with 2009 pandemic influenza confirms that the 2009 pandemic virus can induce severe illness among children and adults, even for those with no underlying medical conditions. The epidemic started almost two months before the usual influenza season in France. No co-circulation of other influenza viruses was identified through the enhanced virological surveillance during the period of data collection.
In our series, the highest ICU admission rate was found in infants and the lowest in the elderly. Being 65 years old or more seems, to be a risk factor for severe disease when hospitalised, but not for death, after adjustment for the presence of co-morbidities. Our results are coherent with other reports on 2009 pandemic influenza. In Australia and New Zealand, the rate of admission to ICU was low in the elderly but the risk of death increased with age [2]. In the analysis of Mexican data, confirmed cases aged 70 years or more, had the lowest mortality rate but the highest death to hospital admission ratio [3]. We did not identify an association for cases between death and being more than 65 years old. This could be explained by the fact that our analysis was adjusted to the presence of co-morbidity. It may also be due to the limited sample size of our series.
The underlying conditions leading to more severe illness we found are those reported in the literature. Chronic respiratory illness is the most prevalent in our case series, as described also by Jain et al. [4], but it is not associated with a higher risk of more severe disease or death among hospitalised cases. In contrast, obesity is clearly a risk factor for severe disease and probably for death as was reported in the literature [2,4,5]. Obesity is a risk factor for severe viral pneumonia [6] while severity connected to chronic respiratory disease is related to the exacerbation of the disease, and is usually responsive to bronchodilatator treatment [7]. Pregnancy, especially at the end of the gestation, is overrepresented among the patients hospitalised and accounts for 7% of admissions to ICU whereas pregnancy (estimated from the number of live birth in 2008 and the number of abortions in France) represents around 1% of the general population. Our finding confirms that pregnancy should be considered as a risk factor for complications from 2009 pandemic influenza [8]. A similar conclusion stands for infants, also accounting for 7% of admissions to ICU.
The interval from the onset of symptoms to admission was longer for severe cases than for non-severe cases. Furthermore, antiviral treatment was initiated less than 48 hours after the onset of symptoms for 74% of non-severe hospitalised cases and 39% for severe cases. As already suggested by data from the United States, it is possible that delayed initiation of antiviral therapy may have contributed to increased severity of illness [4,9]. Communication to patients and physicians should be strengthened on the need for rapid initiation of treatment, whenever indicated.
Of the 244 patients with severe disease, 60 % required ventilator support, 25% had an acute respiratory distress syndrome (ARDS) and 9% required extracorporeal membrane oxygenation (ECMO). Theses results are also consistent with previously published reports [2,4].
Our study has several limitations. Although our surveillance was implemented in the context of public health emergency some cases may have not been reported to InVS. However, several factors are in favour of only few cases having been missed. Firstly, only a few additional cases were identified after cross-checking with data from laboratories. Secondly, cases considered by clinicians as likely to be due to 2009 pandemic influenza, even in the absence of laboratory confirmation, were included in the definition of cases to be notified. Thirdly, regular phone calls with physicians of ICU wards were made by InVS staff in order to complete missing information on received forms and ask for cases not notified. Last but not least, the hospital surveillance is strongly supported by various ICU medical practitioners? societies.
To assess risk factors for severe clinical presentation we used 2009 pandemic influenza cases admitted to medical wards as a control group. This choice of controls may have lead to an underestimation of odds ratios because for some specific population groups potentially more prone to complications such as pregnant women and children, individuals may have been hospitalised as a precautionary measure even in the absence of severe disease. This could explain our finding of a higher proportion of non-severely ill pregnant women hospitalised in medical wards compared to those admitted to ICU.
Our study confirms the role of the underlying conditions as risk factors for severe disease and strengthens the need for a rapid start of antiviral therapy, especially for patients with underlying conditions. Furthermore, it confirms the French national strategy which recommends priority vaccination of pregnant women, close contacts of infants and patients of any age with co-morbidities known to increase the risk of severe influenza.
Our analysis will be renewed when a larger series of cases will be available: as of 2 December, 511 severe cases have been identified with 74 deaths and the epidemic does not seem to have reached its peak yet.
Acknowledgements
We thank all clinicians and the following medical societies: Soci?t? de R?animation de Langue Fran?aise (SRLF), Groupe Francophone de R?animation et Urgences P?diatriques (GFRUP), Soci?t? Fran?aise d'Anesth?sie et de R?animation (SFAR) who were involved in the collection and contribution of clinical data and all laboratories who contributed with RT-PCR results. We also thank all colleagues at InVS who were directly or indirectly involved in the influenza surveillance for their support, especially the regional units of the InVS (CIRES) and we thank Christine Saura and Jean-Claude Desenclos for their advice and support.
<hr>
References
- Vaux S, Bonmarin I, Enouf V, Valette M, Van Der Werf S, Lina B, et al. Cas d'infection par le nouveau virus de la grippe A(H1N1)v en France, situation au 5 juin 2009. BEH 2009. French. Available from: http://www.invs.sante.fr/beh/actuali...gique/r-4.html
- Webb SA, Pettila V, Seppelt I, Bellomo R, Bailey M, Cooper DJ, et al. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. N Engl J Med. 2009;361(20):1925-34.
- Echevarria-Zuno S, Mejia-Arangure JM, Mar-Obeso AJ, Grajales-Muniz C, Robles-Perez E, Gonzalez-Leon M, et al. Infection and death from influenza A H1N1 virus in Mexico: a retrospective analysis. Lancet 2009 Nov 11. [Epub ahead of print]
- Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, et al. Hospitalized Patients with 2009 H1N1 Influenza in the United States, April-June 2009. N Engl J Med. 2009;361(20):1925-44.
- Louie JK, Acosta M, Winter K, Jean C, Gavali S, Schechter R, et al. Factors associated with death or hospitalization due to pandemic 2009 influenza A(H1N1) infection in California. JAMA. 2009;302(17):1896-902.
- Rello J, Rodriguez A, Ibanez P, Socias L, Cebrian J, Marques A, et al. Intensive care adult patients with severe respiratory failure caused by Influenza A (H1N1)v in Spain. Crit Care. 2009;13(5):R148.
- Gordon E, Lazarus SC. Management of chronic obstructive pulmonary disease: Moving beyond the asthma algorithm. J Allergy Clin. Immunol. 2009;124(5):873-80.
- Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, Biggerstaff MS, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet 2009;374(9688):451-8.
- Tr?moli?res F. Les antiviraux de la grippe servent-ils ? quelque chose ? Med Mal Infect. 2009;39:667-73. French.
-
------