 Tweet
Tweet
mBio: Pandemic Paradox - Early Life H2N2 Infection Enhanced Mortality From H1N1pdm09
#13,074
A little over a year ago, in Science: Protection Against Novel Flu Subtypes Via Childhood HA Imprinting,we looked at a study that strongly suggested the first HA Group type influenza virus an individual is exposed to makes the biggest, and most lasting, impression on your immune system.
Today, however, we have a new study in the open-access journal mBio that suggests there is more to this first life exposure to influenza than previously thought.
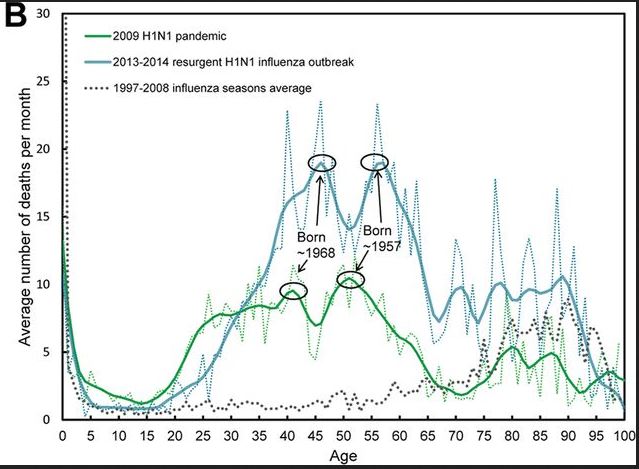
During the 2009 H1N1 pandemic, and its subsequent return for the 2013-14 flu season, those born during the 1957 H2N2 pandemic saw the highest mortality (see mbio chart below).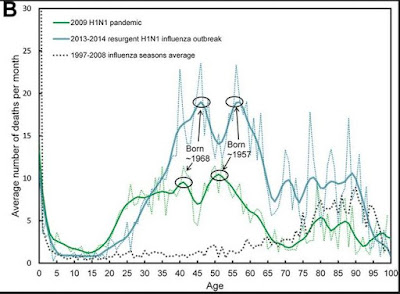
This is doubly unexpected.
H1N1 and H2N2 are both group 1 HA types, and some cross protection might be expected. Also, the mortality rate dropped for those born after 1957 - when H2N2 was still circulating - and didn't spike for those born during the 1968 pandemic when H3N2 (a group 2 HA type) was the only influenza A game in town.
There is some historical precedent for this, as during the 1918 pandemic those born prior to 1890 appear to have been at least partially protected by (an assumed) H1Nx virus that likely circulated prior to the H3Nx pandemic of that year.
Those born in 1890, during the H3Nx pandemic, would have turned 28 in 1918, and as the famous W Curve Chart above illustrates, that is the precise age that saw the highest number of deaths.
Although I'm coming up on my 12th anniversary of full-time flu blogging, I am humbled by how much less I know about influenza than I did when I started.
http://afludiary.blogspot.com/2018/0...life-h2n2.html
 |
|||
| 18 known HA subtypes divided into 2 | groups |
#13,074
A little over a year ago, in Science: Protection Against Novel Flu Subtypes Via Childhood HA Imprinting,we looked at a study that strongly suggested the first HA Group type influenza virus an individual is exposed to makes the biggest, and most lasting, impression on your immune system.
And that the resultant immune response may carry over to other - similar - subtypes within that HA group.
This has some pandemic planning implications since - if your first influenza exposure was to H1N1 or H2N2 (group1) - you may carry some degree of immunity to the H5 viruses (H5N1, H5N6, etc.). If, however, your first exposure was to H3N2 (group 2), you may carry some protection against H7N9 instead.Today, however, we have a new study in the open-access journal mBio that suggests there is more to this first life exposure to influenza than previously thought.
During the 2009 H1N1 pandemic, and its subsequent return for the 2013-14 flu season, those born during the 1957 H2N2 pandemic saw the highest mortality (see mbio chart below).
This is doubly unexpected.
H1N1 and H2N2 are both group 1 HA types, and some cross protection might be expected. Also, the mortality rate dropped for those born after 1957 - when H2N2 was still circulating - and didn't spike for those born during the 1968 pandemic when H3N2 (a group 2 HA type) was the only influenza A game in town.
There is some historical precedent for this, as during the 1918 pandemic those born prior to 1890 appear to have been at least partially protected by (an assumed) H1Nx virus that likely circulated prior to the H3Nx pandemic of that year.
Those born in 1890, during the H3Nx pandemic, would have turned 28 in 1918, and as the famous W Curve Chart above illustrates, that is the precise age that saw the highest number of deaths.
While none of this invalidates the previously described HA Group type cross-protection theory, it does suggest there are exceptions to the rule.
Since I can't possibly do this highly technical and intriguing study justice in the space I have allotted, I heartily suggest you find a quiet corner, turn off your phone ringer for an hour, and immerse yourself in:Pandemic Paradox: Early Life H2N2 Pandemic Influenza Infection Enhanced Susceptibility to Death during the 2009 H1N1 Pandemic
Alain Gagnona,b, Enrique Acostaa, Stacey Hallmanc, Robert Bourbeaua, Lisa Y. Dillona, Nadine Ouellettea, David J. D. Earnd,e, D. Ann Herringf, Kris Inwoodg, Joaquin Madrenash, Matthew S. Millere,i
ABSTRACT
Recent outbreaks of H5, H7, and H9 influenza A viruses in humans have served as a vivid reminder of the potentially devastating effects that a novel pandemic could exert on the modern world. Those who have survived infections with influenza viruses in the past have been protected from subsequent antigenically similar pandemics through adaptive immunity.
Alain Gagnona,b, Enrique Acostaa, Stacey Hallmanc, Robert Bourbeaua, Lisa Y. Dillona, Nadine Ouellettea, David J. D. Earnd,e, D. Ann Herringf, Kris Inwoodg, Joaquin Madrenash, Matthew S. Millere,i
ABSTRACT
Recent outbreaks of H5, H7, and H9 influenza A viruses in humans have served as a vivid reminder of the potentially devastating effects that a novel pandemic could exert on the modern world. Those who have survived infections with influenza viruses in the past have been protected from subsequent antigenically similar pandemics through adaptive immunity.
For example, during the 2009 H1N1 “swine flu” pandemic, those exposed to H1N1 viruses that circulated between 1918 and the 1940s were at a decreased risk for mortality as a result of their previous immunity. It is also generally thought that past exposures to antigenically dissimilar strains of influenza virus may also be beneficial due to cross-reactive cellular immunity. However, cohorts born during prior heterosubtypic pandemics have previously experienced elevated risk of death relative to surrounding cohorts of the same population.
Indeed, individuals born during the 1890 H3Nx pandemic experienced the highest levels of excess mortality during the 1918 “Spanish flu.” Applying Serfling models to monthly mortality and influenza circulation data between October 1997 and July 2014 in the United States and Mexico, we show corresponding peaks in excess mortality during the 2009 H1N1 “swine flu” pandemic and during the resurgent 2013–2014 H1N1 outbreak for those born at the time of the 1957 H2N2 “Asian flu” pandemic.
We suggest that the phenomenon observed in 1918 is not unique and points to exposure to pandemic influenza early in life as a risk factor for mortality during subsequent heterosubtypic pandemics.
IMPORTANCE The relatively low mortality experienced by older individuals during the 2009 H1N1 influenza virus pandemic has been well documented. However, reported situations in which previous influenza virus exposures have enhanced susceptibility are rare and poorly understood. One such instance occurred in 1918—when those born during the heterosubtypic 1890 H3Nx influenza virus pandemic experienced the highest levels of excess mortality.
IMPORTANCE The relatively low mortality experienced by older individuals during the 2009 H1N1 influenza virus pandemic has been well documented. However, reported situations in which previous influenza virus exposures have enhanced susceptibility are rare and poorly understood. One such instance occurred in 1918—when those born during the heterosubtypic 1890 H3Nx influenza virus pandemic experienced the highest levels of excess mortality.
Here, we demonstrate that this phenomenon was not unique to the 1918 H1N1 pandemic but that it also occurred during the contemporary 2009 H1N1 pandemic and 2013–2014 H1N1-dominated season for those born during the heterosubtypic 1957 H2N2 “Asian flu” pandemic.
These data highlight the heretofore underappreciated phenomenon that, in certain instances, prior exposure to pandemic influenza virus strains can enhance susceptibility during subsequent pandemics. These results have important implications for pandemic risk assessment and should inform laboratory studies aimed at uncovering the mechanism responsible for this effect.
(Continue . . . )Although I'm coming up on my 12th anniversary of full-time flu blogging, I am humbled by how much less I know about influenza than I did when I started.
http://afludiary.blogspot.com/2018/0...life-h2n2.html




Comment