 Tweet
Tweet
Quantifying the risk of pandemic influenza in pregnancy and Indigenous people in Australia in 2009 (Euro Surveill., edited)
Eurosurveillance, Volume 14, Issue 50, 17 December 2009
Rapid communications
Quantifying the risk of pandemic influenza in pregnancy and Indigenous people in Australia in 2009
H Kelly ( )<sup>1</sup>, G N Mercer<sup>2</sup>, A C Cheng<sup>3</sup>
)<sup>1</sup>, G N Mercer<sup>2</sup>, A C Cheng<sup>3</sup>
<hr> Citation style for this article: Kelly H, Mercer GN, Cheng AC. Quantifying the risk of pandemic influenza in pregnancy and Indigenous people in Australia in 2009. Euro Surveill. 2009;14(50):pii=19441. Available online: http://www.eurosurveillance.org/View...rticleId=19441
Date of submission: 03 December 2009
<hr> An increased relative risk of infection with the 2009 pandemic H1N1 influenza virus associated with pregnancy and Indigenous status has been a common finding in many countries. Using publicly available data from May to October 2009 in Australia, we estimated the relative risk of hospitalisation, admission to intensive care unit and death as 5.2, 6.5 and 1.4 respectively for pregnant women, and as 6.6, 6.2 and 5.2, respectively for Indigenous Australians. Pregnancy and Indigenous status were associated with severe influenza. More complete analyses of risks in these groups are required to understand and prevent influenza morbidity and mortality.
<hr>Introduction The 2009 H1N1 influenza pandemic in Australia corresponded with the expected influenza season, although pandemic virus circulation began relatively early. In the populous states of New South Wales and Victoria, pandemic influenza virus circulated for about 10-13 weeks [1,2]. The death rate due to pandemic H1N1 influenza was reported as approximately 9 per million for Australia, in the middle of the range of 5-15 per million that was reported for other populous countries in the southern hemisphere [3]. Groups most at risk in the pandemic were recognised to be Indigenous people, pregnant women, the morbidly obese and people with recognised comorbidities [4]. Before the end of the 2009 pandemic in Australia, we used publicly available data to estimate the increased risk of hospitalisation for pregnant women as 3.2 (95% confidence interval (CI): 2.6 to 4.1) [5]. We now use the same data sources to provide estimates of the relative risk of hospitalisation, intensive care unit (ICU) admission and death for pregnant and Indigenous Australians throughout the entire pandemic period.
Methods
We obtained population data from the Australian Bureau of Statistics [6]. Data extracted included estimated total population in 2009, population by sex and age group, estimated number of live births and proportion of the Australian population identifying themselves as Aboriginal or Torres Strait Islanders (Indigenous Australians). We obtained data on the hospitalisations, ICU admissions and deaths in pregnant women and Indigenous Australians due to pandemic H1N1 influenza from reports published by the Australian Department of Health and Ageing [7].
We estimated the cumulative incidence of all outcomes for the entire pandemic period, from May to October 2009. To estimate the relative risk (RR) for the two nominated risk groups, we compared the cumulative incidence of each outcome in the risk group with the same outcome in the entire population minus the estimated population in the risk group. Confidence intervals for RR were calculated using the method outlined in Bland and Altman [8]. We estimated the number of at-risk pregnant women as previously described by using the fertility and abortion rates in women aged 15-44 years [5] and compared this number with the estimated number of live births in 2009. We used the estimate of the proportion of Indigenous Australians in 2009 from the projected Australian census data.
Results
Our previous estimate of at-risk pregnant women in Australia was 237,215 and equivalent to about 1.1% of the Australian population [5]. The minimum prevalence of pregnancy should be 40 weeks divided by 52 weeks multiplied by 296,600, which is the estimated number of live births for 2008 [9] and the estimate we used for the number of live births in 2009. The fraction of live births represents the expected duration of pregnancy and leads to a minimum estimate of the number of pregnant women in Australia which was 228,154. The proportion of the Australian population who identify themselves as Aboriginal or Torres Strait islanders is estimated as 2.5%, i.e. 534,350 Indigenous Australians [10]. This estimate attempts to correct for under counting in census data and we could find no more exact estimate of the number of Indigenous Australians.
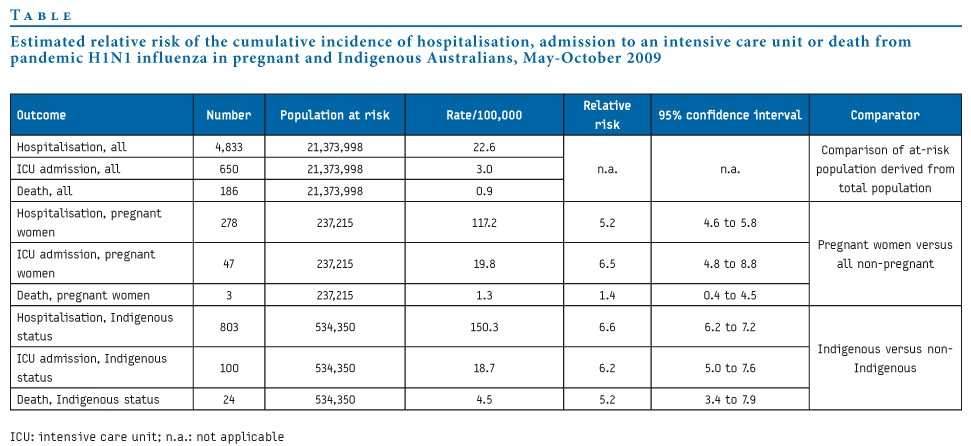
More than 4,800 hospitalisations, 650 admissions to ICU and almost 200 deaths due to pandemic H1N1 influenza were reported in Australia between May and October 2009. Estimations of the RR of hospitalisation, ICU admission and death for pregnant and Indigenous Australians ranged between 5.2 and 6.6, with the exception of the RR for death in pregnant women, which was only 1.4 (95% CI: 0.3 to 4.3). This imprecise estimate was based on only three deaths (see Table). We also calculated the RR of hospitalisation in pregnant women compared with not pregnant women of reproductive age (15-44 years). Of an estimated 4,492,701 women of reproductive age, 1,030 were hospitalised. This gave an RR of 5.1 (95% CI: 4.5 to 5.8), similar to the comparison with the general population.
Table. Estimated relative risk of the cumulative incidence of hospitalisation, admission to an intensive care unit or death from pandemic H1N1 influenza in pregnant and Indigenous Australians, May-October 2009

Our estimate of pregnant women at risk was 3.8% higher than the minimum number of pregnant women estimated from the number of live births. Using the minimum estimate of pregnancy did not change RR estimates for pregnancy to any appreciable degree (data not shown).
Discussion
Before the end of the 2009 pandemic in Australia, we had estimated the RR for hospitalisation of pregnant women due to pandemic H1N1 influenza as approximately 3.2 [5], comparable to an early estimate from the United States of 4.3 [11]. At the end of the 2009 pandemic in Australia, this risk appeared to be higher, of the order of 5.2. We had not previously estimated the increased risks associated with Indigenous status. These risks appear to be at least as high as the risk associated with pregnancy, with a much higher risk for death in Indigenous Australians (RR=5.2) compared with pregnant women (RR=1.4).
Limitations of these results include the potential under-ascertainment of cases, but this is more likely for those perceived not at increased risk (the denominator) than those at increased risk, pregnant and Indigenous Australians (the numerator). For the entire pandemic period, efforts were concentrated in identifying pandemic H1N1 influenza in vulnerable population groups, and testing was also prioritised for hospitalised patients. Increased ascertainment of the group perceived not to be at risk would result in lower estimates of RR than we have reported. We therefore think it is unlikely that our estimates of RR for any of the outcomes are spuriously low. A further limitation of the reported RR estimates results from necessarily imprecise estimates of the at-risk populations. Moreover, with access only to data in the public domain, we could not report age-stratified or age-adjusted rates or adjust for the presence of co-morbidities. A more thorough analysis of risk is warranted, with risk during pregnancy stratified by gestational age.
In a 2008 review of influenza vaccination in pregnancy, Mak and colleagues concluded that during severe influenza seasons and the pandemics of 1918-19 and 1957-58, pregnant women were at increased risk of influenza-related hospital admission compared with not pregnant women or women post-partum [12]. They also noted that the risk rose with increasing gestation and the presence of co-morbidities. A study from Tennessee between 1974 and 1993 found the excess rates of hospitalisation of pregnant women for an acute cardio-respiratory illness in the second trimester to be 6.3 and in the third trimester 10.8 per 10,000 healthy woman-months. Much lower estimates of excess hospitalisation rates, in the range of 0.4-2.0 per 10,000 healthy woman-months, were reported for influenza-attributable hospital admissions 1990-2002 in Nova Scotia [12]. Reflecting the non-systematic approach to risk quantification in the influenza literature, none of the reported risks were due to laboratory-confirmed disease. In a more recent systematic review of influenza immunisation in pregnancy, Skowronski and De Serres confirmed that studies using laboratory-confirmed outcomes are scarce [13]. This lack of quality data continues to frustrate our understanding of the burden of influenza and prevents direct comparison with the data presented here [5].
Point estimates for RR, defined as the incidence rate ratio, of up to 3.8 for hospital admission coded as influenza in Aboriginal children in Western Australia between 1996-2005 have recently been made (personal communication, Hannah Moore, Telethon Institute for Child Health Research, Perth, Western Australia). This outcome is more specific than the outcomes studied in pregnant women but again is not strictly comparable to the data presented here.
While it is generally accepted that both pregnancy and Indigenous status increase the risk of adverse outcomes due to laboratory-confirmed influenza, quantification of these risks is surprisingly scarce. We have provided estimates of RR from data available in the public domain from the Australian pandemic of 2009, but acknowledge the need for more complete analyses.
Acknowledgements
We thank the surveillance and epidemiology staff from the Australian Department of Health and Ageing who have been responsible for the production of the quality pandemic influenza surveillance reports published online.
GN Mercer was partially funded by an Australian Government National Health and Medical Research Council (NHMRC) Capacity Building Grant (3651073). AC Cheng is supported by a NHMRC Health Professionals Training Fellowship (400481).
<hr>References
-
------
Eurosurveillance, Volume 14, Issue 50, 17 December 2009
Rapid communications
Quantifying the risk of pandemic influenza in pregnancy and Indigenous people in Australia in 2009
H Kelly (
- Victorian Infectious Diseases Reference Laboratory and School of Population Health, University of Melbourne, Melbourne, Australia
- National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australia
- Department of Epidemiology and Preventive Medicine, Monash University Melbourne, Australia
<hr> Citation style for this article: Kelly H, Mercer GN, Cheng AC. Quantifying the risk of pandemic influenza in pregnancy and Indigenous people in Australia in 2009. Euro Surveill. 2009;14(50):pii=19441. Available online: http://www.eurosurveillance.org/View...rticleId=19441
Date of submission: 03 December 2009
<hr> An increased relative risk of infection with the 2009 pandemic H1N1 influenza virus associated with pregnancy and Indigenous status has been a common finding in many countries. Using publicly available data from May to October 2009 in Australia, we estimated the relative risk of hospitalisation, admission to intensive care unit and death as 5.2, 6.5 and 1.4 respectively for pregnant women, and as 6.6, 6.2 and 5.2, respectively for Indigenous Australians. Pregnancy and Indigenous status were associated with severe influenza. More complete analyses of risks in these groups are required to understand and prevent influenza morbidity and mortality.
<hr>Introduction The 2009 H1N1 influenza pandemic in Australia corresponded with the expected influenza season, although pandemic virus circulation began relatively early. In the populous states of New South Wales and Victoria, pandemic influenza virus circulated for about 10-13 weeks [1,2]. The death rate due to pandemic H1N1 influenza was reported as approximately 9 per million for Australia, in the middle of the range of 5-15 per million that was reported for other populous countries in the southern hemisphere [3]. Groups most at risk in the pandemic were recognised to be Indigenous people, pregnant women, the morbidly obese and people with recognised comorbidities [4]. Before the end of the 2009 pandemic in Australia, we used publicly available data to estimate the increased risk of hospitalisation for pregnant women as 3.2 (95% confidence interval (CI): 2.6 to 4.1) [5]. We now use the same data sources to provide estimates of the relative risk of hospitalisation, intensive care unit (ICU) admission and death for pregnant and Indigenous Australians throughout the entire pandemic period.
Methods
We obtained population data from the Australian Bureau of Statistics [6]. Data extracted included estimated total population in 2009, population by sex and age group, estimated number of live births and proportion of the Australian population identifying themselves as Aboriginal or Torres Strait Islanders (Indigenous Australians). We obtained data on the hospitalisations, ICU admissions and deaths in pregnant women and Indigenous Australians due to pandemic H1N1 influenza from reports published by the Australian Department of Health and Ageing [7].
We estimated the cumulative incidence of all outcomes for the entire pandemic period, from May to October 2009. To estimate the relative risk (RR) for the two nominated risk groups, we compared the cumulative incidence of each outcome in the risk group with the same outcome in the entire population minus the estimated population in the risk group. Confidence intervals for RR were calculated using the method outlined in Bland and Altman [8]. We estimated the number of at-risk pregnant women as previously described by using the fertility and abortion rates in women aged 15-44 years [5] and compared this number with the estimated number of live births in 2009. We used the estimate of the proportion of Indigenous Australians in 2009 from the projected Australian census data.
Results
Our previous estimate of at-risk pregnant women in Australia was 237,215 and equivalent to about 1.1% of the Australian population [5]. The minimum prevalence of pregnancy should be 40 weeks divided by 52 weeks multiplied by 296,600, which is the estimated number of live births for 2008 [9] and the estimate we used for the number of live births in 2009. The fraction of live births represents the expected duration of pregnancy and leads to a minimum estimate of the number of pregnant women in Australia which was 228,154. The proportion of the Australian population who identify themselves as Aboriginal or Torres Strait islanders is estimated as 2.5%, i.e. 534,350 Indigenous Australians [10]. This estimate attempts to correct for under counting in census data and we could find no more exact estimate of the number of Indigenous Australians.
More than 4,800 hospitalisations, 650 admissions to ICU and almost 200 deaths due to pandemic H1N1 influenza were reported in Australia between May and October 2009. Estimations of the RR of hospitalisation, ICU admission and death for pregnant and Indigenous Australians ranged between 5.2 and 6.6, with the exception of the RR for death in pregnant women, which was only 1.4 (95% CI: 0.3 to 4.3). This imprecise estimate was based on only three deaths (see Table). We also calculated the RR of hospitalisation in pregnant women compared with not pregnant women of reproductive age (15-44 years). Of an estimated 4,492,701 women of reproductive age, 1,030 were hospitalised. This gave an RR of 5.1 (95% CI: 4.5 to 5.8), similar to the comparison with the general population.
Table. Estimated relative risk of the cumulative incidence of hospitalisation, admission to an intensive care unit or death from pandemic H1N1 influenza in pregnant and Indigenous Australians, May-October 2009
Our estimate of pregnant women at risk was 3.8% higher than the minimum number of pregnant women estimated from the number of live births. Using the minimum estimate of pregnancy did not change RR estimates for pregnancy to any appreciable degree (data not shown).
Discussion
Before the end of the 2009 pandemic in Australia, we had estimated the RR for hospitalisation of pregnant women due to pandemic H1N1 influenza as approximately 3.2 [5], comparable to an early estimate from the United States of 4.3 [11]. At the end of the 2009 pandemic in Australia, this risk appeared to be higher, of the order of 5.2. We had not previously estimated the increased risks associated with Indigenous status. These risks appear to be at least as high as the risk associated with pregnancy, with a much higher risk for death in Indigenous Australians (RR=5.2) compared with pregnant women (RR=1.4).
Limitations of these results include the potential under-ascertainment of cases, but this is more likely for those perceived not at increased risk (the denominator) than those at increased risk, pregnant and Indigenous Australians (the numerator). For the entire pandemic period, efforts were concentrated in identifying pandemic H1N1 influenza in vulnerable population groups, and testing was also prioritised for hospitalised patients. Increased ascertainment of the group perceived not to be at risk would result in lower estimates of RR than we have reported. We therefore think it is unlikely that our estimates of RR for any of the outcomes are spuriously low. A further limitation of the reported RR estimates results from necessarily imprecise estimates of the at-risk populations. Moreover, with access only to data in the public domain, we could not report age-stratified or age-adjusted rates or adjust for the presence of co-morbidities. A more thorough analysis of risk is warranted, with risk during pregnancy stratified by gestational age.
In a 2008 review of influenza vaccination in pregnancy, Mak and colleagues concluded that during severe influenza seasons and the pandemics of 1918-19 and 1957-58, pregnant women were at increased risk of influenza-related hospital admission compared with not pregnant women or women post-partum [12]. They also noted that the risk rose with increasing gestation and the presence of co-morbidities. A study from Tennessee between 1974 and 1993 found the excess rates of hospitalisation of pregnant women for an acute cardio-respiratory illness in the second trimester to be 6.3 and in the third trimester 10.8 per 10,000 healthy woman-months. Much lower estimates of excess hospitalisation rates, in the range of 0.4-2.0 per 10,000 healthy woman-months, were reported for influenza-attributable hospital admissions 1990-2002 in Nova Scotia [12]. Reflecting the non-systematic approach to risk quantification in the influenza literature, none of the reported risks were due to laboratory-confirmed disease. In a more recent systematic review of influenza immunisation in pregnancy, Skowronski and De Serres confirmed that studies using laboratory-confirmed outcomes are scarce [13]. This lack of quality data continues to frustrate our understanding of the burden of influenza and prevents direct comparison with the data presented here [5].
Point estimates for RR, defined as the incidence rate ratio, of up to 3.8 for hospital admission coded as influenza in Aboriginal children in Western Australia between 1996-2005 have recently been made (personal communication, Hannah Moore, Telethon Institute for Child Health Research, Perth, Western Australia). This outcome is more specific than the outcomes studied in pregnant women but again is not strictly comparable to the data presented here.
While it is generally accepted that both pregnancy and Indigenous status increase the risk of adverse outcomes due to laboratory-confirmed influenza, quantification of these risks is surprisingly scarce. We have provided estimates of RR from data available in the public domain from the Australian pandemic of 2009, but acknowledge the need for more complete analyses.
Acknowledgements
We thank the surveillance and epidemiology staff from the Australian Department of Health and Ageing who have been responsible for the production of the quality pandemic influenza surveillance reports published online.
GN Mercer was partially funded by an Australian Government National Health and Medical Research Council (NHMRC) Capacity Building Grant (3651073). AC Cheng is supported by a NHMRC Health Professionals Training Fellowship (400481).
<hr>References
- Fielding JE, Higgins N, Gregory JE, Grant KA, Catton MG, Bergerei I, et al. Pandemic H1N1 influenza in Victoria, April-September 2009. Euro Surveill. 2009;14(42):pii=19368. Available from: http://www.eurosurveillance.org/View...rticleId=19368
- New South Wales public health network. Progression and impact of the first winter wave of the 2009 pandemic H1N1 influenza in New South Wales, Australia. Euro Surveill. 2009;14(42):pii=19365. Available from: http://www.eurosurveillance.org/View...rticleId=19365
- Baker MG, Kelly H, Wilson N. Pandemic H1N1 influenza lessons from the southern hemisphere. Euro Surveill 2009;14(42):pii=19370. Available from: http://www.eurosurveillance.org/View...rticleId=19370
- ANZIC Influenza Investigators, Webb SA, Pettil? V, Seppelt I, Bellomo R, Bailey M, et al. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. New Engl J Med. 2009;361(20):1925-34.
- Kelly H. A pandemic response to a disease of predominantly seasonal intensity. Med J Aust. Rapid Online Publication 16 November 2009. Available from: http://www.mja.com.au/public/issues/...l11025_fm.html
- Australian Bureau of Statistics. Population by Age and Sex, Australian States and Territories, June 2008. Australian Bureau of Statistics; 2009 December 9. Available from: http://www.abs.gov.au/Ausstats/abs@.nsf/mf/3201.0
- Australian Government. Australian Influenza Surveillance Reports. Report 27, 2009. Available from: http://www.healthemergency.gov.au/in...-no27-2009.pdf
- Bland JM, Altman D. Statistics Notes: The odds ratio. BMJ. 2000;320(7247):1468.
- Australian Bureau of Statistics. 3301.0 - Births, Australia, 2008. Australian Bureau of Statistics; 2009 November 11. Available from: http://www.abs.gov.au/AUSSTATS/abs@.nsf/mf/3301.0
- Australian Bureau of Statistics. 4705.0 - Population Distribution, Aboriginal and Torres Strait Islander Australians, 2006. Australian Bureau of Statistics; 2007 August 15. Available from: http://www.abs.gov.au/AUSSTATS/abs@....6?OpenDocument
- Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, Biggerstaff MS, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374(9688):451-8.
- Mak TK, Mangtani P, Leese J, Watson JM, Pfeifer D. Influenza vaccination in pregnancy: current evidence and selected national policies. Lancet Infect Dis. 2008;8(1):44-52.
- Skowronski DM, De Serres G. Is routine influenza immunization warranted in early pregnancy? Vaccine. 2009;27(35):4754-70.
-
------