 Tweet
Tweet
hat tip Laidback Al
A Review of Human Influenza A(H5N1) Cases in 2013
In 2013, 38 human cases of Influenza A(H5N1) were reported from around the world. This number represents an 18% increase over the number of reported cases in 2012. Six countries reported cases in 2013, Bangladesh, Cambodia, China, Egypt, Indonesia, and Vietnam. Cambodia reported about 71% (27) of all cases reported in 2013. In 2013, children younger than 10 years old represent about 63% of all cases. No human clusters were reported in 2013. Relative to other countries, Cambodia experienced the greatest percentage increase in human infections in a short period of time. The continued low frequency of reported infections does not eliminate H5N1 as a pandemic threat.
Influenza A(H5N1), (often referred to ?bird flu? or avian influenza or HPAI), is an emerging infectious disease. It was first detected in humans in Hong Kong in 1997. Since 2003, the World Health Organization (WHO) has been monitoring human outbreaks of H5N1. Through December 31, 2013, WHO has officially reported a total of 648 confirmed human cases of H5N1. The most current WHO summary report on H5N1 is Influenza at the human-animal interface: Summary and assessment as of 20 December 2013. The most recent WHO time line of significant events associated with the H5N1 virus was last updated on December 17, 2012 (link).The following summary of human cases of H5N1 in 2013 is generally organized according to the outline presented previously in ?H5N1 in 2012: The Year in Review?. (link)
Since 2003, 15 countries have reported human H5N1 cases to WHO (link). The count of WHO-confirmed H5N1 cases in 2013 is 38. Compared to 2012, the number of H5N1 cases increased by about 18%. In 2013, 6 countries reported human cases of H5N1, Bangladesh (1 case), Cambodia (26), China (2), Egypt (4), Indonesia (3), and Vietnam (2). These same six countries were the only countries to report H5N1 cases in 2012.
Geographic Distribution
More than 60% of the H5N1 cases reported in 2012 occurred in Egypt and Indonesia. In 2013, more than 60% of the H5N1 cases were reported from Cambodia. Between 2003 and 2012, Cambodia had only reported 21 cases. In the 12 month period of 2013, Cambodia reported 26 H5N1 cases, more than doubling the count of previously reported cases. Indonesia continues to lead the world in cumulative number of reported human H5N1 cases with 195. Egypt is second with 173 reported cases. Based on the total number of cases reported, Cambodia now exceeds China and Thailand in total count of cases. It now ranks fourth behind Indonesia, Egypt, and Vietnam.
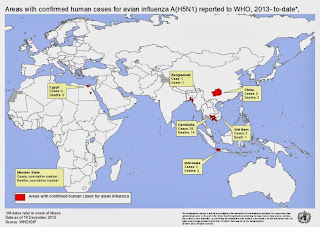
Map: WHO map of countries (Administrative level 1) with human H5N1 cases in 2013.
Map: All countries reporting human H5N1 cases since 2003.

Map: The approximate geolocations of H5N1 cases in Cambodia from 2003-2013. 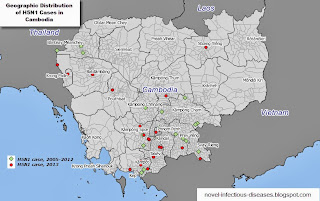
Gender Statistics
Of the 38 reported cases in 2013 19 were male and 19 were female, although in the past females outnumbered males among reported cases. Overall, females represent about 53% of all of the WHO-reported H5N1 cases where sex was noted. In 2013, 12 of the males died as did an equal number of females (12).
Age Statistics
In 2013, the age of H5N1 cases ranged from less than one year old to 58 years old with a median age of 6. Children under 10 years old were the most commonly infected individuals. Twenty-four (63%) of the 38 cases were less than 10 years old in age.
Graph: Comparison of H5N1 infections in 2012 and 2013 by age group.

Twenty-two of the 24 children in 2013 were reported from Cambodia. Only two other children were reported, a four-year-old from Vietnam and a one-year-old from Bangladesh. Among all H5N1 cases, the greatest number cases are children in the 0-10-years-old age group.
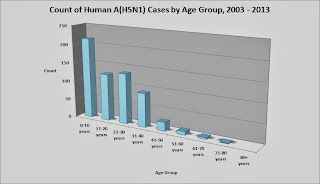
Graph: All H5N1 cases by age group, 2003 to 2013.
Mortality Statistics
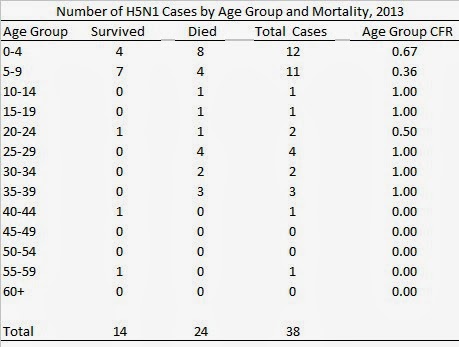
Of the 38 cases in 2013, 24 died. The case-fatality ratio (CFR) is .625 for the 2013 calendar year. Over the past several years the CFR has not appreciably decreased. Although there is inter-year variability, the overall CFR for the 648 WHO reported cases is .59.
As in previous years, children continued to have a slightly better survival rate than infected adults. The CFR for the 24 children under 10 years old is .54, while the CFR for the 14 individuals older than 10 years is .78.
With the 26 cases and 14 deaths, Cambodia now has the second highest CFR rate at .70. Among the countries reporting at least 25 H5N1 cases, only Indonesia, with a CFR of .84, exceeds the CFR in Cambodia.
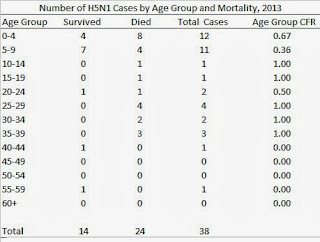
Table: H5N1 mortality by age group in 2013.
Seasonality
As noted previously, human H5N1 cases do not randomly occur throughout the year, but the number of cases fluctuates in a pattern similar to that of seasonal influenza in the northern hemisphere (link). Below is a current graph of the month of onset for almost all of the worldwide confirmed cases since 2009.
Graph: Monthly H5N1 case count, 2009 to 2013.

H5N1 Clusters
All 38 cases reported to WHO in 2013 represent sporadic cases. No clusters, as defined by WHO, were identified in 2013. A cluster is defined as two or more cases of confirmed, probable, or suspected Influenza A(H5N1) infections with onset of illness occurring within the same two-week period and who are in the same geographical area and/or are epidemiologically linked. (link)
Discussion
In summary, the 38 H5N1 cases reported in 2013 is a slight increase over 2012, but less than the highest yearly total of 115 cases in 2006. The concentration of 27 cases in Cambodia including 24 infected children is unusual, and the lack of reported clusters in 2103 is notable as well. As noted in 2012, there has been an observable trend of an increasing number of H5N1 infections among young children. That trend has continued in 2013 with 63 % of the cases being younger than 10 years old. Previous analyses suggested that this age group had a high recovery rate. However, the infected children in 2013 had much lower survival rate. The reason for low recovery rates in children in Cambodia deserved further research.
Gain of function research in 2011 demonstrated that, in theory, only a few genetic changes are necessary for H5N1 to become an aerosolized pandemic virus. While media attention in 2013 has focused on the Middle East respiratory syndrome coronavirus and the novel influenza virus A(H7N9), H5N1 continues to a pandemic threat, even if it is not receiving media attention.
Acknowledgements and Notes
I thank all of the internet sources, posters at FluTrackers.com, and other internet disease trackers for their online efforts to follow and track H5N1 cases. Thanks are also due to open source journals and researchers who post full copies of their papers and data sets.
The data and information used here have been derived from numerous publicly available sources including WHO, various ministries of health, internet bloggers, internet forums, and other media reports available online through December 31, 2013. For some individual cases, specific details are lacking or conflicting information is presented in online reports. However, the information and graphics presented here are based on data which is believed to be reasonably accurate and current through December 31, 2013.
Posted by Laidback Al at <a class="timestamp-link" href="http://novel-infectious-diseases.blogspot.com/2014/01/a-review-of-human-influenza-ah5n1-cases.html" rel="bookmark" title="permanent link"><abbr class="published" itemprop="datePublished" title="2014-01-01T11:07:00-08:00">11:07 AM</abbr>
A Review of Human Influenza A(H5N1) Cases in 2013
In 2013, 38 human cases of Influenza A(H5N1) were reported from around the world. This number represents an 18% increase over the number of reported cases in 2012. Six countries reported cases in 2013, Bangladesh, Cambodia, China, Egypt, Indonesia, and Vietnam. Cambodia reported about 71% (27) of all cases reported in 2013. In 2013, children younger than 10 years old represent about 63% of all cases. No human clusters were reported in 2013. Relative to other countries, Cambodia experienced the greatest percentage increase in human infections in a short period of time. The continued low frequency of reported infections does not eliminate H5N1 as a pandemic threat.
Influenza A(H5N1), (often referred to ?bird flu? or avian influenza or HPAI), is an emerging infectious disease. It was first detected in humans in Hong Kong in 1997. Since 2003, the World Health Organization (WHO) has been monitoring human outbreaks of H5N1. Through December 31, 2013, WHO has officially reported a total of 648 confirmed human cases of H5N1. The most current WHO summary report on H5N1 is Influenza at the human-animal interface: Summary and assessment as of 20 December 2013. The most recent WHO time line of significant events associated with the H5N1 virus was last updated on December 17, 2012 (link).The following summary of human cases of H5N1 in 2013 is generally organized according to the outline presented previously in ?H5N1 in 2012: The Year in Review?. (link)
Since 2003, 15 countries have reported human H5N1 cases to WHO (link). The count of WHO-confirmed H5N1 cases in 2013 is 38. Compared to 2012, the number of H5N1 cases increased by about 18%. In 2013, 6 countries reported human cases of H5N1, Bangladesh (1 case), Cambodia (26), China (2), Egypt (4), Indonesia (3), and Vietnam (2). These same six countries were the only countries to report H5N1 cases in 2012.
Geographic Distribution
More than 60% of the H5N1 cases reported in 2012 occurred in Egypt and Indonesia. In 2013, more than 60% of the H5N1 cases were reported from Cambodia. Between 2003 and 2012, Cambodia had only reported 21 cases. In the 12 month period of 2013, Cambodia reported 26 H5N1 cases, more than doubling the count of previously reported cases. Indonesia continues to lead the world in cumulative number of reported human H5N1 cases with 195. Egypt is second with 173 reported cases. Based on the total number of cases reported, Cambodia now exceeds China and Thailand in total count of cases. It now ranks fourth behind Indonesia, Egypt, and Vietnam.
Map: WHO map of countries (Administrative level 1) with human H5N1 cases in 2013.

Map: All countries reporting human H5N1 cases since 2003.

Map: The approximate geolocations of H5N1 cases in Cambodia from 2003-2013.

Gender Statistics
Of the 38 reported cases in 2013 19 were male and 19 were female, although in the past females outnumbered males among reported cases. Overall, females represent about 53% of all of the WHO-reported H5N1 cases where sex was noted. In 2013, 12 of the males died as did an equal number of females (12).
Age Statistics
In 2013, the age of H5N1 cases ranged from less than one year old to 58 years old with a median age of 6. Children under 10 years old were the most commonly infected individuals. Twenty-four (63%) of the 38 cases were less than 10 years old in age.
Graph: Comparison of H5N1 infections in 2012 and 2013 by age group.

Twenty-two of the 24 children in 2013 were reported from Cambodia. Only two other children were reported, a four-year-old from Vietnam and a one-year-old from Bangladesh. Among all H5N1 cases, the greatest number cases are children in the 0-10-years-old age group.
Graph: All H5N1 cases by age group, 2003 to 2013.

Mortality Statistics
Of the 38 cases in 2013, 24 died. The case-fatality ratio (CFR) is .625 for the 2013 calendar year. Over the past several years the CFR has not appreciably decreased. Although there is inter-year variability, the overall CFR for the 648 WHO reported cases is .59.
As in previous years, children continued to have a slightly better survival rate than infected adults. The CFR for the 24 children under 10 years old is .54, while the CFR for the 14 individuals older than 10 years is .78.
With the 26 cases and 14 deaths, Cambodia now has the second highest CFR rate at .70. Among the countries reporting at least 25 H5N1 cases, only Indonesia, with a CFR of .84, exceeds the CFR in Cambodia.
Table: H5N1 mortality by age group in 2013.
Seasonality
As noted previously, human H5N1 cases do not randomly occur throughout the year, but the number of cases fluctuates in a pattern similar to that of seasonal influenza in the northern hemisphere (link). Below is a current graph of the month of onset for almost all of the worldwide confirmed cases since 2009.
Graph: Monthly H5N1 case count, 2009 to 2013.

H5N1 Clusters
All 38 cases reported to WHO in 2013 represent sporadic cases. No clusters, as defined by WHO, were identified in 2013. A cluster is defined as two or more cases of confirmed, probable, or suspected Influenza A(H5N1) infections with onset of illness occurring within the same two-week period and who are in the same geographical area and/or are epidemiologically linked. (link)
Discussion
In summary, the 38 H5N1 cases reported in 2013 is a slight increase over 2012, but less than the highest yearly total of 115 cases in 2006. The concentration of 27 cases in Cambodia including 24 infected children is unusual, and the lack of reported clusters in 2103 is notable as well. As noted in 2012, there has been an observable trend of an increasing number of H5N1 infections among young children. That trend has continued in 2013 with 63 % of the cases being younger than 10 years old. Previous analyses suggested that this age group had a high recovery rate. However, the infected children in 2013 had much lower survival rate. The reason for low recovery rates in children in Cambodia deserved further research.
Gain of function research in 2011 demonstrated that, in theory, only a few genetic changes are necessary for H5N1 to become an aerosolized pandemic virus. While media attention in 2013 has focused on the Middle East respiratory syndrome coronavirus and the novel influenza virus A(H7N9), H5N1 continues to a pandemic threat, even if it is not receiving media attention.
Acknowledgements and Notes
I thank all of the internet sources, posters at FluTrackers.com, and other internet disease trackers for their online efforts to follow and track H5N1 cases. Thanks are also due to open source journals and researchers who post full copies of their papers and data sets.
The data and information used here have been derived from numerous publicly available sources including WHO, various ministries of health, internet bloggers, internet forums, and other media reports available online through December 31, 2013. For some individual cases, specific details are lacking or conflicting information is presented in online reports. However, the information and graphics presented here are based on data which is believed to be reasonably accurate and current through December 31, 2013.
Posted by Laidback Al at <a class="timestamp-link" href="http://novel-infectious-diseases.blogspot.com/2014/01/a-review-of-human-influenza-ah5n1-cases.html" rel="bookmark" title="permanent link"><abbr class="published" itemprop="datePublished" title="2014-01-01T11:07:00-08:00">11:07 AM</abbr>
Comment