 Tweet
Tweet
High prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus in the Norwegian population following a major epidemic and a large vaccination campaign in autumn 2009 (Euro Surveill., abstract, edited)
[Source: Eurosurveillance.org, full article (LINK). Edited.]
Eurosurveillance, Volume 15, Issue 31, 05 August 2010
Rapid communications
High prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus in the Norwegian population following a major epidemic and a large vaccination campaign in autumn 2009
K Waalen<sup>1</sup>, A Kilander<sup>1</sup>, S G Dudman<sup>1</sup>, G H Krogh<sup>1</sup>, T Aune<sup>1</sup>, O Hungnes ( )<sup>1</sup>
)<sup>1</sup>
<hr>
Citation style for this article: Waalen K, Kilander A, Dudman SG, Krogh GH, Aune T, Hungnes O. High prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus in the Norwegian population following a major epidemic and a large vaccination campaign in autumn 2009. Euro Surveill. 2010;15(31):pii=19633. Available online: http://www.eurosurveillance.org/View...rticleId=19633
Date of submission: 30 June 2010
<hr>
The prevalence of antibodies reactive to the 2009 pandemic influenza A(H1N1) was determined in sera collected before the start of the pandemic, during the early phase, and after the main epidemic wave and nationwide vaccination campaign in Norway. A substantial rise in prevalence of antibodies at protective titres, from 3.2% to 44.9%, was observed between August 2009 and January 2010. The highest prevalence, 65.3%, was seen in the age group of 10-19 year-olds.
<hr>
Introduction
A new influenza virus in humans emerged in the spring of 2009 in Mexico. The virus was identified to be a triple reassorted A(H1N1) variant of swine origin but with a still unknown reservoir. Due to the wide spread of the virus around the globe the World Health Organization (WHO) declared within a few weeks the first pandemic of the 21st century. In Norway, the first cases of 2009 pandemic influenza A(H1N1) virus infections were recorded in early May. Until mid-summer, cases were scattered and they were almost exclusively travellers from abroad and their contacts. A minor epidemic occurred from late July to early August, with a high but gradually declining proportion of travel-related cases. This was followed by a comparatively calm period leading up to a major influenza epidemic during October and November 2009, surpassing all previous peaks recorded in the current Norwegian clinical influenza surveillance system which monitors influenza-like illness consultation rates and has been in operation since 1998 [1]. This wave culminated in early November and largely subsided by the end of 2009. Subsequent influenza activity from January to May 2010 has been unusually low.
The 2009 pandemic influenza A(H1N1) surveillance and vaccination in Norway
Virological influenza surveillance in Norway is based on reporting from diagnostic laboratories to the Norwegian Institute for Public Health (NIPH). During the pandemic period, laboratories performed virus detection through reverse transcription?polymerase chain reaction (RT-PCR) in the great majority of cases, with a small minority done through virus isolation or antigen detection. Based on virologically-confirmed cases notified to the NIPH, the highest impact of the epidemic was among the younger age groups (Figure 1).
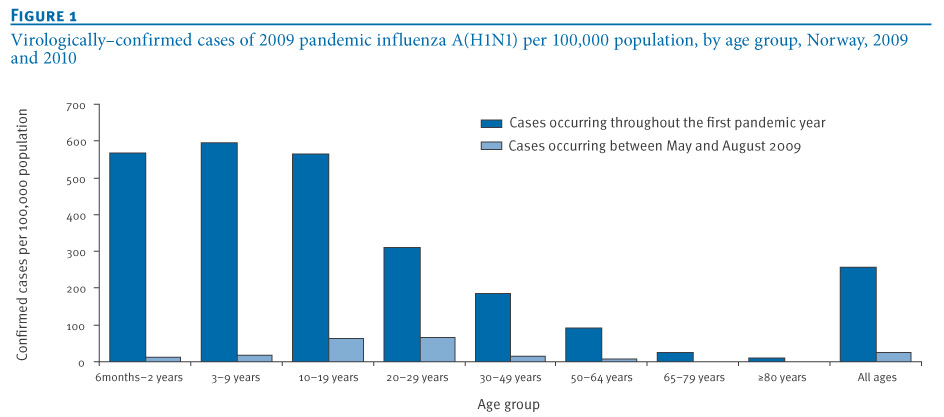
Figure 1. Virologically-confirmed cases of 2009 pandemic influenza A(H1N1) per 100,000 population, by age group, Norway, 2009 and 2010
The recorded incidence declined with increasing age; less than 10% of the confirmed cases were aged 50 years or above, and less than 2% were aged 65 years or above. By week 36 in 2009, after the first small pandemic wave in July?August, the majority of confirmed cases were seen in the age groups of 10?19 year?olds and 20?29 year?olds (34% and 34%, respectively). The age groups under the age of 10 years became more prominent during the main pandemic wave in autumn, increasing from 10% to 27% of all confirmed cases. Similar age patterns were seen when looking at positivity rates within age groups (per cent of specimens testing positive; data not shown), indicating that the patterns were not strongly distorted by testing biases.
As part of the national pandemic preparedness, Norwegian health authorities had entered an advance purchase agreement that secured the country a population-wide supply of monovalent adjuvanted vaccine in case of a pandemic. When deliveries of Pandemrix (GlaxoSmithKline Biologicals s.a.) commenced in mid-October 2009, a large-scale vaccination campaign was launched. Designated priority risk groups and exposed healthcare workers were vaccinated first. Then the general population was offered the vaccine, beginning with the younger age groups, particularly children below school-age, school-age children and adolescents. The great majority of vaccinated individuals received one dose with the exception of immunocompromised persons, and, to some extent, children under ten years of age for whom a two-dose recommendation was given initially. Vaccinated individuals were recorded in the national vaccination registry, SYSVAK. Preliminary data indicate that around 40% of the Norwegian population (approximately 1.9 million people) have been recorded as vaccinated, varying from 25% for the age group of 20-29 year-olds up to 52% for the age group of six months-two year-olds and 57% for three-nine year?olds. For the other age groups, the vaccination coverage figures are within the range 35%?46%. The majority of recorded vaccinations (>95%) was carried out from October to December 2009. However, the present SYSVAK records are not considered to be complete, and a provisional estimate of 2.2 million people (45% of the population) vaccinated is being used by the Norwegian Health authorities (B Feiring, personal communication June 2010).
Serological survey during the pandemic
Since the late 1970s, an annual serosurvey of antibodies reactive to contemporary influenza viruses has been carried out in Norway [2,3]. The annual serum panel is collected in August each year, consisting of approximately 2,200 age- and geographically representative residual sera from hospital laboratories. The information regarding each serum is limited to patient age and sex, and county of residence. Serum antibody titres were determined using the haemagglutination?inhibition (HI) test [4], testing sera in serial two-fold dilutions starting at dilution 1:20, with turkey red blood cells (RBC) as indicator cells. A HI titre of 40 or higher is considered protective against the test virus strain, while sera with HI titre of 20 or more were counted as seropositive.
The serum panel collected in August 2009 (n=2,116) was analysed for antibodies reactive to the pandemic reference virus A/California/07/2009 (H1N1v) in addition to the preceding winter?s seasonal influenza viruses (data not shown). Viral antigen was grown in embryonated chicken eggs and used non-inactivated. In January 2010, a supplementary serum panel (n=541) was collected from five hospital laboratories across Norway. Like the main panel, these sera were also representative for the various age groups. The January 2010 panel was collected in the wake of a major influenza epidemic, and, in order to avoid over-representation of influenza cases, laboratories were asked to exclude sera which had been submitted due to respiratory illness.
In addition, a subset of the serum panel collected in August 2008 (n=689), representative for all age groups and counties across the country, was tested for HI reactivity to the pandemic influenza virus in order to determine the background level of pre-existing antibodies reactive to this virus.
Results and discussion
The results of the HI analysis for various serum panels are shown in Figure 2 (A?C) and in the Table.
Figure 2. Frequency of seropositivity and seroprotection to 2009 pandemic influenza A(H1N1) virus in sera collected in Norway in (A) August 2008, (B) August 2009, and (C) January 2010

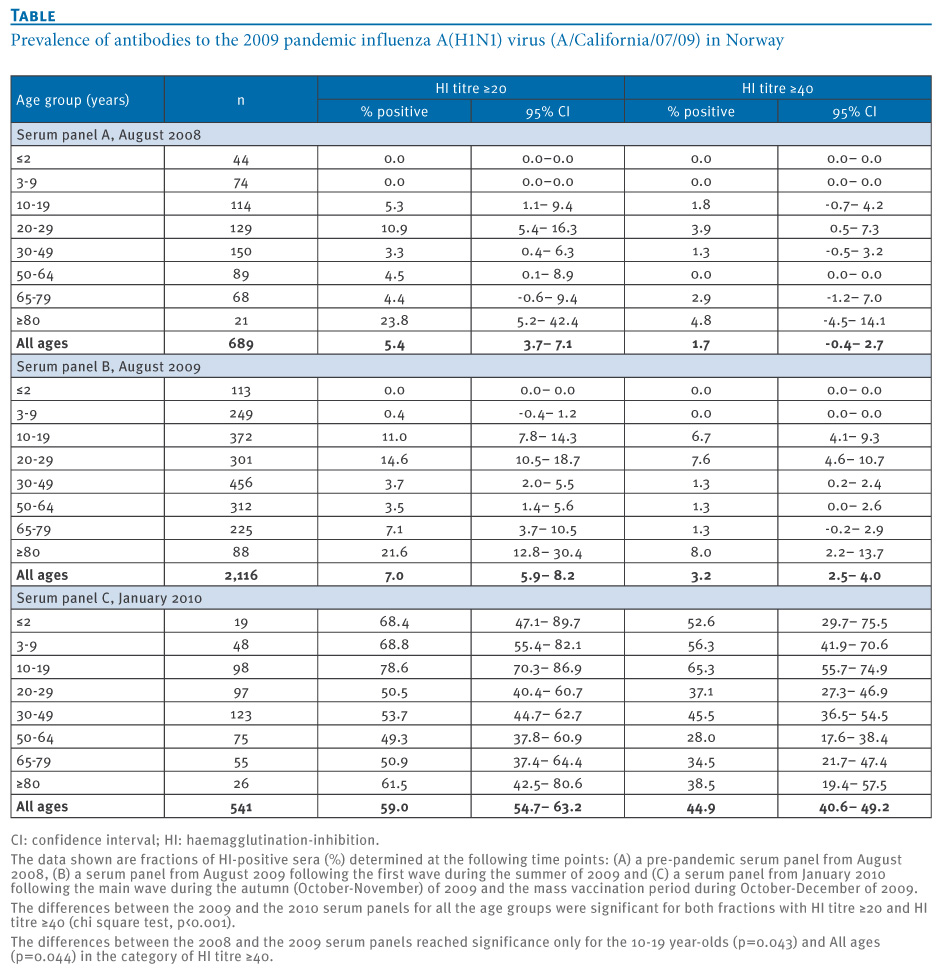
Table. Prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus (A/California/07/09) in Norway

The data for the 2008 serum panel show that there was a low frequency of pre-existing protective antibodies to the 2009 pandemic influenza A(H1N1) virus (1.7%, all ages, HI ≥40). The highest frequency was seen in people over 80 years of age (4.8%). Interestingly, pre-existing antibodies at titres correlating with protection were also seen in adolescents (10-19 years) and young adults (20-29 years) with frequencies of 1.8% and 3.9%, respectively. The nature of pre-existing antibodies reactive to the pandemic influenza virus in this age segment is unclear since exposure to viruses resembling the pandemic strain is unlikely, and further investigation is warranted. Detectable antibodies (HI≥20) were seen in all age groups except for children under the age of ten years (Table). In the elderly, those born before 1950, and in particular those older than 80 years, cross-reactive antibodies might be due to earlier infection with influenza viruses sharing similar antigenic epitopes with the current pandemic influenza virus as suggested in recent reports [5,6]. In these studies, various levels of pre-existing cross-reactive antibodies to the 2009 pandemic influenza A(H1N1) virus were found.
In August 2009 the prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus shows only minor differences from the pre-pandemic 2008 baseline level (Figure 2B). This may be an indication that the early wave in the summer of 2009 was too small to substantially influence the immunity at population level. However, during May?August, confirmed cases in Norway were mainly in adolescents and young adults (Figure 1), and a slight increase in seropositivity in that age segment (significant only for the group of 10?19 year?olds, p<0.05) may reflect immunity acquired from recent infection. Contrary to the situation in the United Kingdom [7], few cases were seen in children under school age and in school age children at that time, possibly because the school vacation in Norway spans from late June until late August, thus limiting the scope for effective transmission of virus in the age groups below 15-20 years of age during summer. In the August 2009 serum panel, the overall prevalence across age groups of titres 40 or above for the seasonal H1N1 virus A/Brisbane/59/2007 was 13%. The age pattern of seasonal influenza A(H1N1) seroprevalence was somewhat more skewed towards younger persons, and a large percentage (44%) of sera with protective titres to the pandemic virus was not reactive to the current seasonal influenza A(H1N1) vaccine strain (data not shown). This probably indicates that the observed reactivity to pandemic influenza A(H1N1) prior to the pandemic cannot be explained solely as cross-reactivity of antibodies raised in response to recent seasonal viruses.
A substantial and significant increase in overall prevalence of protective antibodies (HI titre ≥40) to the pandemic 2009 A(H1N1) influenza virus was observed from August 2009 to January 2010, from 3.2% to 44.9% (p<0.001) (Figure 2, Table). Similarly, all age groups showed a significant increase in the prevalence of detectable as well as protective antibodies. The frequency of protective antibodies was particularly high in persons under 20 years of age (61.2%, 95% confidence interval (CI): 53,6 % ?68,8%), while 74.5% (95% CI: 67.8%?81.3%) had detectable antibodies (titre ≥20). In people aged 20 years and older the figures were substantially lower, 37.8% (95% CI: 32.8%?42.8%) and 52.1% (95% CI: 47.0%?57.3%), respectively. In particular, the 50-64 year-olds age group had the lowest prevalence of protective antibody in January 2010 (28.0%) despite recorded vaccination coverage of about 43%. A higher proportion (49.3%) had detectable antibodies. The incidence of laboratory-confirmed infections was comparatively low in this age group (Figure 1). Conceivably, the immune response to vaccination or infection in this age group resulted in antibodies that were only partially directed against the pandemic strain, possibly due to the phenomenon of original antigenic sin [8]. A similar pattern was also seen in the age group 65-79 year-olds, but to a somewhat lesser extent.
Our sera from January 2010 were collected approximately four to six weeks after the main pandemic wave had subsided, and also after the main drive of a nationwide vaccination campaign with a population vaccine uptake probably well exceeding 40%. The vaccination status of the serum donors is not known, therefore our analysis cannot differentiate between seropositivity resulting from infection, from immunisation, or from a combination of the two.
Our data are thus less suitable for estimating the extent of infection than corresponding studies performed in populations with a lower vaccination coverage [9,10]. In light of age patterns of infection and vaccination, infection is likely to have contributed most to the rise in immunity in the 20-29-year-olds who had the lowest recorded vaccine uptake. Conversely, vaccination might have contributed most to the rise in the elderly who appear to have been spared of widespread infection. Our data furthermore indicate that immunity in the population against the pandemic virus has risen substantially. Approximately 45% of the population has antibodies at a level corresponding to protection and an additional 15% of the population has detectable antibodies at lower titres which may also offer some protection. This observed level of population immunity may prove to be sufficient to prevent a new pandemic wave of high magnitude. However, lesser outbreaks cannot be excluded, and antigenic drift of the virus might impair the protective effect. Furthermore, it is not known how well the observed immunity to the pandemic virus will be sustained.
Conclusions
A substantial increase in antibodies against pandemic 2009 A(H1N1) influenza virus was observed in population representative serum panels in Norway between August 2009 and January 2010. This is consistent with recorded high incidence of infection and a high rate of vaccine uptake, both taking place during October?December 2009. Provided that this level of immunity does not wane substantially, and that the antigenic properties of the virus do not change significantly, the high population immunity may prove sufficient to prevent large-scale epidemics of the pandemic influenza virus in Norway in the upcoming influenza season.
Acknowledgements
We would like to thank laboratories in the following hospitals for their invaluable contribution in providing the sera used in the present study: ?stfold Hospital/Fredrikstad; Akershus University Hospital; Oslo University Hospital, Innlandet Hospital/Lillehammer; Buskerud Hospital/Drammen; Vestfold Hospital/T?nsberg; Unilabs Telelab AS/Skien; S?rlandet Hospital/Kristiansand; Stavanger University Hospital, Haukeland University Hospital/Bergen; F?rde Central Hospital; Molde Hospital; St.Olav Hospital, Trondheim; Levanger Hospital; Nordlandssykehuset/Bod?; University Hospital of North Norway/Troms?, Hammerfest Hospital. The WHO Collaborating Centre at the National Institute for Medical Research, London, UK, is gratefully acknowledged for providing virus and ferret control serum used in the HI test. The Department for Infectious Disease Epidemiology and Department of Vaccinology at NIPH are gratefully acknowledged for contributing incidence and vaccination data, respectively. We further thank the staff of the influenza laboratory, Department of Virology, NIPH; Valentina Johansen, Anne Marie Lund, Marianne Morken, and Remilyn Ramos?Ocao for excellent technical assistance.
<hr>
References
-
-------
[Source: Eurosurveillance.org, full article (LINK). Edited.]
Eurosurveillance, Volume 15, Issue 31, 05 August 2010
Rapid communications
High prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus in the Norwegian population following a major epidemic and a large vaccination campaign in autumn 2009
K Waalen<sup>1</sup>, A Kilander<sup>1</sup>, S G Dudman<sup>1</sup>, G H Krogh<sup>1</sup>, T Aune<sup>1</sup>, O Hungnes (
- Department of Virology, Norwegian Institute of Public Health, Oslo, Norway
<hr>
Citation style for this article: Waalen K, Kilander A, Dudman SG, Krogh GH, Aune T, Hungnes O. High prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus in the Norwegian population following a major epidemic and a large vaccination campaign in autumn 2009. Euro Surveill. 2010;15(31):pii=19633. Available online: http://www.eurosurveillance.org/View...rticleId=19633
Date of submission: 30 June 2010
<hr>
The prevalence of antibodies reactive to the 2009 pandemic influenza A(H1N1) was determined in sera collected before the start of the pandemic, during the early phase, and after the main epidemic wave and nationwide vaccination campaign in Norway. A substantial rise in prevalence of antibodies at protective titres, from 3.2% to 44.9%, was observed between August 2009 and January 2010. The highest prevalence, 65.3%, was seen in the age group of 10-19 year-olds.
<hr>
Introduction
A new influenza virus in humans emerged in the spring of 2009 in Mexico. The virus was identified to be a triple reassorted A(H1N1) variant of swine origin but with a still unknown reservoir. Due to the wide spread of the virus around the globe the World Health Organization (WHO) declared within a few weeks the first pandemic of the 21st century. In Norway, the first cases of 2009 pandemic influenza A(H1N1) virus infections were recorded in early May. Until mid-summer, cases were scattered and they were almost exclusively travellers from abroad and their contacts. A minor epidemic occurred from late July to early August, with a high but gradually declining proportion of travel-related cases. This was followed by a comparatively calm period leading up to a major influenza epidemic during October and November 2009, surpassing all previous peaks recorded in the current Norwegian clinical influenza surveillance system which monitors influenza-like illness consultation rates and has been in operation since 1998 [1]. This wave culminated in early November and largely subsided by the end of 2009. Subsequent influenza activity from January to May 2010 has been unusually low.
The 2009 pandemic influenza A(H1N1) surveillance and vaccination in Norway
Virological influenza surveillance in Norway is based on reporting from diagnostic laboratories to the Norwegian Institute for Public Health (NIPH). During the pandemic period, laboratories performed virus detection through reverse transcription?polymerase chain reaction (RT-PCR) in the great majority of cases, with a small minority done through virus isolation or antigen detection. Based on virologically-confirmed cases notified to the NIPH, the highest impact of the epidemic was among the younger age groups (Figure 1).
Figure 1. Virologically-confirmed cases of 2009 pandemic influenza A(H1N1) per 100,000 population, by age group, Norway, 2009 and 2010
The recorded incidence declined with increasing age; less than 10% of the confirmed cases were aged 50 years or above, and less than 2% were aged 65 years or above. By week 36 in 2009, after the first small pandemic wave in July?August, the majority of confirmed cases were seen in the age groups of 10?19 year?olds and 20?29 year?olds (34% and 34%, respectively). The age groups under the age of 10 years became more prominent during the main pandemic wave in autumn, increasing from 10% to 27% of all confirmed cases. Similar age patterns were seen when looking at positivity rates within age groups (per cent of specimens testing positive; data not shown), indicating that the patterns were not strongly distorted by testing biases.
As part of the national pandemic preparedness, Norwegian health authorities had entered an advance purchase agreement that secured the country a population-wide supply of monovalent adjuvanted vaccine in case of a pandemic. When deliveries of Pandemrix (GlaxoSmithKline Biologicals s.a.) commenced in mid-October 2009, a large-scale vaccination campaign was launched. Designated priority risk groups and exposed healthcare workers were vaccinated first. Then the general population was offered the vaccine, beginning with the younger age groups, particularly children below school-age, school-age children and adolescents. The great majority of vaccinated individuals received one dose with the exception of immunocompromised persons, and, to some extent, children under ten years of age for whom a two-dose recommendation was given initially. Vaccinated individuals were recorded in the national vaccination registry, SYSVAK. Preliminary data indicate that around 40% of the Norwegian population (approximately 1.9 million people) have been recorded as vaccinated, varying from 25% for the age group of 20-29 year-olds up to 52% for the age group of six months-two year-olds and 57% for three-nine year?olds. For the other age groups, the vaccination coverage figures are within the range 35%?46%. The majority of recorded vaccinations (>95%) was carried out from October to December 2009. However, the present SYSVAK records are not considered to be complete, and a provisional estimate of 2.2 million people (45% of the population) vaccinated is being used by the Norwegian Health authorities (B Feiring, personal communication June 2010).
Serological survey during the pandemic
Since the late 1970s, an annual serosurvey of antibodies reactive to contemporary influenza viruses has been carried out in Norway [2,3]. The annual serum panel is collected in August each year, consisting of approximately 2,200 age- and geographically representative residual sera from hospital laboratories. The information regarding each serum is limited to patient age and sex, and county of residence. Serum antibody titres were determined using the haemagglutination?inhibition (HI) test [4], testing sera in serial two-fold dilutions starting at dilution 1:20, with turkey red blood cells (RBC) as indicator cells. A HI titre of 40 or higher is considered protective against the test virus strain, while sera with HI titre of 20 or more were counted as seropositive.
The serum panel collected in August 2009 (n=2,116) was analysed for antibodies reactive to the pandemic reference virus A/California/07/2009 (H1N1v) in addition to the preceding winter?s seasonal influenza viruses (data not shown). Viral antigen was grown in embryonated chicken eggs and used non-inactivated. In January 2010, a supplementary serum panel (n=541) was collected from five hospital laboratories across Norway. Like the main panel, these sera were also representative for the various age groups. The January 2010 panel was collected in the wake of a major influenza epidemic, and, in order to avoid over-representation of influenza cases, laboratories were asked to exclude sera which had been submitted due to respiratory illness.
In addition, a subset of the serum panel collected in August 2008 (n=689), representative for all age groups and counties across the country, was tested for HI reactivity to the pandemic influenza virus in order to determine the background level of pre-existing antibodies reactive to this virus.
Results and discussion
The results of the HI analysis for various serum panels are shown in Figure 2 (A?C) and in the Table.
Figure 2. Frequency of seropositivity and seroprotection to 2009 pandemic influenza A(H1N1) virus in sera collected in Norway in (A) August 2008, (B) August 2009, and (C) January 2010
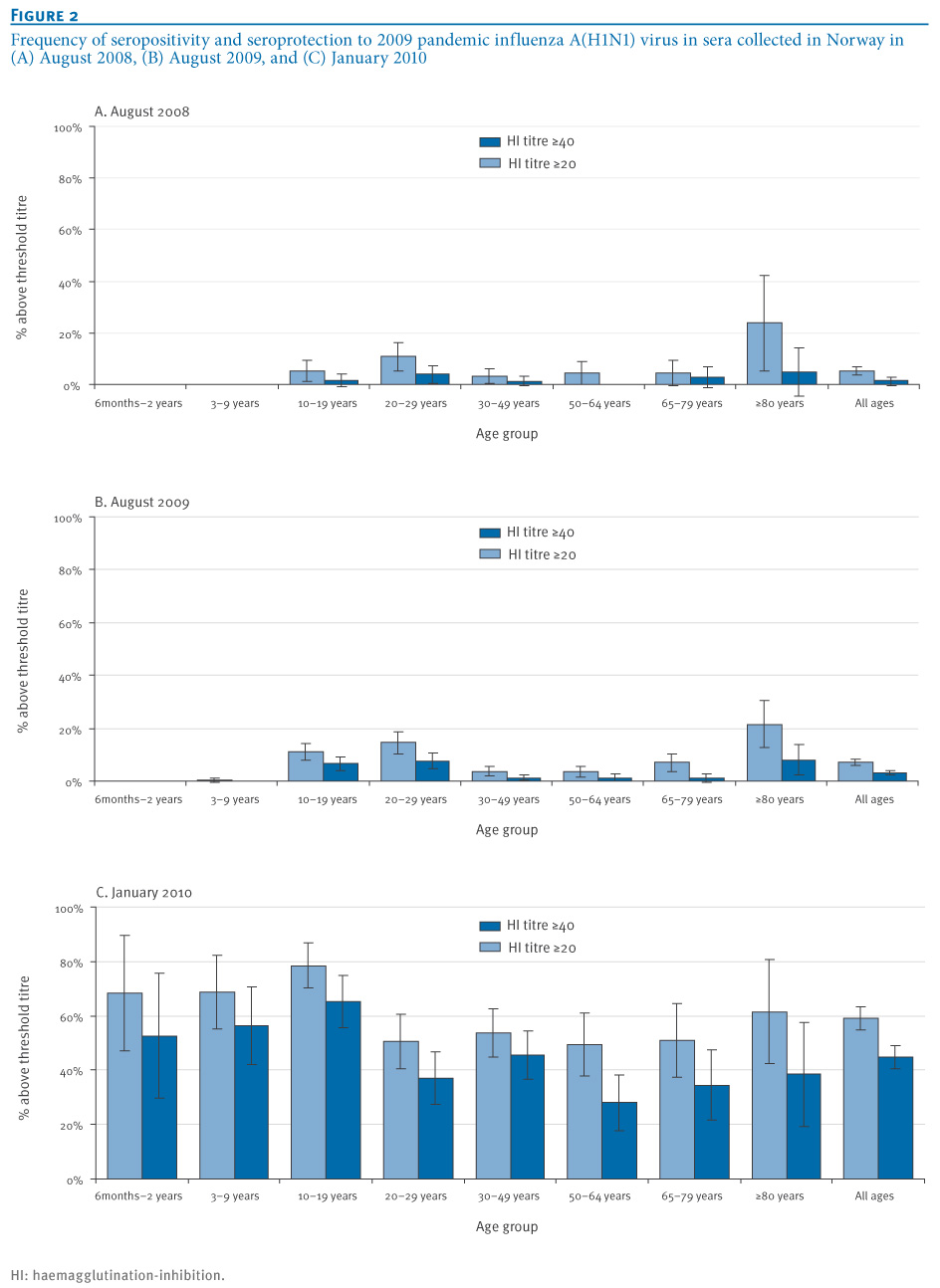
Table. Prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus (A/California/07/09) in Norway
The data for the 2008 serum panel show that there was a low frequency of pre-existing protective antibodies to the 2009 pandemic influenza A(H1N1) virus (1.7%, all ages, HI ≥40). The highest frequency was seen in people over 80 years of age (4.8%). Interestingly, pre-existing antibodies at titres correlating with protection were also seen in adolescents (10-19 years) and young adults (20-29 years) with frequencies of 1.8% and 3.9%, respectively. The nature of pre-existing antibodies reactive to the pandemic influenza virus in this age segment is unclear since exposure to viruses resembling the pandemic strain is unlikely, and further investigation is warranted. Detectable antibodies (HI≥20) were seen in all age groups except for children under the age of ten years (Table). In the elderly, those born before 1950, and in particular those older than 80 years, cross-reactive antibodies might be due to earlier infection with influenza viruses sharing similar antigenic epitopes with the current pandemic influenza virus as suggested in recent reports [5,6]. In these studies, various levels of pre-existing cross-reactive antibodies to the 2009 pandemic influenza A(H1N1) virus were found.
In August 2009 the prevalence of antibodies to the 2009 pandemic influenza A(H1N1) virus shows only minor differences from the pre-pandemic 2008 baseline level (Figure 2B). This may be an indication that the early wave in the summer of 2009 was too small to substantially influence the immunity at population level. However, during May?August, confirmed cases in Norway were mainly in adolescents and young adults (Figure 1), and a slight increase in seropositivity in that age segment (significant only for the group of 10?19 year?olds, p<0.05) may reflect immunity acquired from recent infection. Contrary to the situation in the United Kingdom [7], few cases were seen in children under school age and in school age children at that time, possibly because the school vacation in Norway spans from late June until late August, thus limiting the scope for effective transmission of virus in the age groups below 15-20 years of age during summer. In the August 2009 serum panel, the overall prevalence across age groups of titres 40 or above for the seasonal H1N1 virus A/Brisbane/59/2007 was 13%. The age pattern of seasonal influenza A(H1N1) seroprevalence was somewhat more skewed towards younger persons, and a large percentage (44%) of sera with protective titres to the pandemic virus was not reactive to the current seasonal influenza A(H1N1) vaccine strain (data not shown). This probably indicates that the observed reactivity to pandemic influenza A(H1N1) prior to the pandemic cannot be explained solely as cross-reactivity of antibodies raised in response to recent seasonal viruses.
A substantial and significant increase in overall prevalence of protective antibodies (HI titre ≥40) to the pandemic 2009 A(H1N1) influenza virus was observed from August 2009 to January 2010, from 3.2% to 44.9% (p<0.001) (Figure 2, Table). Similarly, all age groups showed a significant increase in the prevalence of detectable as well as protective antibodies. The frequency of protective antibodies was particularly high in persons under 20 years of age (61.2%, 95% confidence interval (CI): 53,6 % ?68,8%), while 74.5% (95% CI: 67.8%?81.3%) had detectable antibodies (titre ≥20). In people aged 20 years and older the figures were substantially lower, 37.8% (95% CI: 32.8%?42.8%) and 52.1% (95% CI: 47.0%?57.3%), respectively. In particular, the 50-64 year-olds age group had the lowest prevalence of protective antibody in January 2010 (28.0%) despite recorded vaccination coverage of about 43%. A higher proportion (49.3%) had detectable antibodies. The incidence of laboratory-confirmed infections was comparatively low in this age group (Figure 1). Conceivably, the immune response to vaccination or infection in this age group resulted in antibodies that were only partially directed against the pandemic strain, possibly due to the phenomenon of original antigenic sin [8]. A similar pattern was also seen in the age group 65-79 year-olds, but to a somewhat lesser extent.
Our sera from January 2010 were collected approximately four to six weeks after the main pandemic wave had subsided, and also after the main drive of a nationwide vaccination campaign with a population vaccine uptake probably well exceeding 40%. The vaccination status of the serum donors is not known, therefore our analysis cannot differentiate between seropositivity resulting from infection, from immunisation, or from a combination of the two.
Our data are thus less suitable for estimating the extent of infection than corresponding studies performed in populations with a lower vaccination coverage [9,10]. In light of age patterns of infection and vaccination, infection is likely to have contributed most to the rise in immunity in the 20-29-year-olds who had the lowest recorded vaccine uptake. Conversely, vaccination might have contributed most to the rise in the elderly who appear to have been spared of widespread infection. Our data furthermore indicate that immunity in the population against the pandemic virus has risen substantially. Approximately 45% of the population has antibodies at a level corresponding to protection and an additional 15% of the population has detectable antibodies at lower titres which may also offer some protection. This observed level of population immunity may prove to be sufficient to prevent a new pandemic wave of high magnitude. However, lesser outbreaks cannot be excluded, and antigenic drift of the virus might impair the protective effect. Furthermore, it is not known how well the observed immunity to the pandemic virus will be sustained.
Conclusions
A substantial increase in antibodies against pandemic 2009 A(H1N1) influenza virus was observed in population representative serum panels in Norway between August 2009 and January 2010. This is consistent with recorded high incidence of infection and a high rate of vaccine uptake, both taking place during October?December 2009. Provided that this level of immunity does not wane substantially, and that the antigenic properties of the virus do not change significantly, the high population immunity may prove sufficient to prevent large-scale epidemics of the pandemic influenza virus in Norway in the upcoming influenza season.
Acknowledgements
We would like to thank laboratories in the following hospitals for their invaluable contribution in providing the sera used in the present study: ?stfold Hospital/Fredrikstad; Akershus University Hospital; Oslo University Hospital, Innlandet Hospital/Lillehammer; Buskerud Hospital/Drammen; Vestfold Hospital/T?nsberg; Unilabs Telelab AS/Skien; S?rlandet Hospital/Kristiansand; Stavanger University Hospital, Haukeland University Hospital/Bergen; F?rde Central Hospital; Molde Hospital; St.Olav Hospital, Trondheim; Levanger Hospital; Nordlandssykehuset/Bod?; University Hospital of North Norway/Troms?, Hammerfest Hospital. The WHO Collaborating Centre at the National Institute for Medical Research, London, UK, is gratefully acknowledged for providing virus and ferret control serum used in the HI test. The Department for Infectious Disease Epidemiology and Department of Vaccinology at NIPH are gratefully acknowledged for contributing incidence and vaccination data, respectively. We further thank the staff of the influenza laboratory, Department of Virology, NIPH; Valentina Johansen, Anne Marie Lund, Marianne Morken, and Remilyn Ramos?Ocao for excellent technical assistance.
<hr>
References
- The Norwegian Institute of Public Health (NIPH). Influenza. Oslo: NIPH. [Accessed: 4 Aug 2010]. Norwegian. Available from: http://www.fhi.no/influensa
- Haaheim LR. Surveillance of the antibody status to current influenza strains in the Norwegian population. 1: Method of serum sampling and evaluation of the A/USSR/77 (H1N1) impact in various age groups in 1978. NIPH Ann. 1979;2(2):45?54.
- Haaheim LR. Surveillance of the antibody status to current influenza strains in the Norwegian population. 2: Antibodies to the A/USSR/90/77 (H1N1) virus in various age groups after the second epidemic wave. NIPH Ann. 1980;3(1):49?56.
- Kendal AP, Pereira MS, Skehel JJ, editors. Concepts and procedures for laboratory?based influenza surveillance. Atlanta: Center for Disease Control and Prevention; 1982.
- Rizzo C, Rota MC, Bella A, Alfonsi V, Declich S, Caporali MG, et al. Cross-reactive antibody responses to the 2009 A/H1N1v influenza virus in the Italian population in the pre-pandemic period. Vaccine. 2010;28(20):3558-62.
- World Health Organization (WHO). Seroepidemiological studies of pandemic influenza A (H1N1)2009 virus. Wkly Epidemiol Rec. 2010;85(24):229-35.
- Miller E, Hoschler K, Hardelid P, Stanford E, Andrews N, Zambon M. Incidence of 2009 pandemic influenza A H1N1 infection in England: a cross?sectional serological study. Lancet. 2010;375(9720):1100-8.
- Adalja AA, Henderson DA. Original antigenic sin and pandemic (H1N1) 2009. Emerg Infec Dis. 2010;16(6):1028?9.
- Zimmer SM, Crevar CJ, Carter DM, Stark JH, Giles BM, Zimmerman RK, et al. Seroprevalence following the second wave of Pandemic 2009 H1N1 influenza in Pittsburgh, PA, USA. PLoS One. 2010;5(7):e11601.
- Adamson WE, Maddi S, Robertson C, McDonagh S, Molyneaux PJ, Templeton KE, et al. 2009 pandemic influenza A(H1N1) virus in Scotland: geographically variable immunity in Spring 2010, following the winter outbreak. Euro Surveill. 2010;15(24):pii=19590. Available from: http://www.eurosurveillance.org/View...rticleId=19590
-
-------