 Tweet
Tweet
Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April ? 3 October 2009 (Euro Surveill., edited)
Eurosurveillance, Volume 14, Issue 44, 05 November 2009
Rapid communications
Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April ? 3 October 2009
G Cullen<sup>1</sup>, J Martin ( )<sup>1</sup>, J O?Donnell<sup>1</sup>, M Boland<sup>2</sup>, M Canny<sup>3</sup>, E. Keane<sup>4</sup>, A McNamara<sup>5</sup>, A O?Hora<sup>1</sup>, M Fitzgerald<sup>1</sup>, S Jackson<sup>1</sup>, D Igoe<sup>1</sup>, D O?Flanagan<sup>1</sup>
)<sup>1</sup>, J O?Donnell<sup>1</sup>, M Boland<sup>2</sup>, M Canny<sup>3</sup>, E. Keane<sup>4</sup>, A McNamara<sup>5</sup>, A O?Hora<sup>1</sup>, M Fitzgerald<sup>1</sup>, S Jackson<sup>1</sup>, D Igoe<sup>1</sup>, D O?Flanagan<sup>1</sup>
<hr> Citation style for this article: Cullen G, Martin J, O?Donnell J, Boland M, Canny M, Keane E, McNamara A, O?Hora A, Fitzgerald M, Jackson S, Igoe D, O?Flanagan D. Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April ? 3 October 2009. Euro Surveill. 2009;14(44):pii=19389. Available online: LINK
Date of submission: 19 October 2009
<hr> From 28 April 2009 to 3 October 2009, 205 cases of confirmed pandemic H1N1 influenza were hospitalised in Ireland. Detailed case-based epidemiological information was gathered on all hospitalised cases. Age-specific hospitalisation rates were highest in the age group of 15 to 19 year-olds and lowest in those aged 65 years and over. Nineteen hospitalised cases (9%) were admitted to intensive care units (ICU) where the median length of stay was 24 days. Four hospitalised cases (2%) died. Fifty-one percent of hospitalised cases and 42% of ICU cases were not in a recognised risk group. Asthma was the most common risk factor among cases; however, people with haemoglobinopathies and immunosuppression were the most over-represented groups.
<hr>Introduction In late April 2009, a novel influenza virus led to human infection in Mexico and the United States (US) and subsequently spread worldwide. On 11 June, 2009, the World Health Organization (WHO) declared a phase 6 pandemic of moderate severity [1].
The first case of pandemic influenza in Ireland was diagnosed on 28 April 2009. Existing surveillance systems were augmented and enhanced case-based surveillance of pandemic H1N1 influenza was commenced. Until mid-July, all cases of influenza were actively followed up; most cases were imported, mainly from the US, the majority were in young adults and there were few hospitalisations [2]. On 16 July Ireland moved to mitigation, and detailed case-based surveillance was confined to hospitalised cases. Influenza-like illness (ILI) presentations to sentinel general practices remained below the seasonal threshold (17.8/100,000) between April and mid-July [3]. By late July, the ILI rate reached 35 per 100,000 population and fluctuated around this level until mid-September. Since then ILI rates have risen, reaching 87.3 per 100,000 population in the week ending 3 October [3].
The WHO has recommended that countries undertake case-based surveillance on the first 200 hospitalised cases, as it is important to identify those most at risk of adverse outcomes, hospitalisation and death due to pandemic H1N1 influenza. To date, there is limited research on risk factors associated with adverse outcomes in Europe [4-11] and therefore, we report on the enhanced case-based surveillance of the first 205 hospitalised cases of confirmed pandemic H1N1 influenza in Ireland.
Methods
Enhanced surveillance was undertaken on all cases of confirmed pandemic H1N1 influenza deemed to require admission to hospital for management of their illness by the treating clinician. Regional Departments of Public Health or the treating hospital clinician completed the enhanced surveillance form. Data collected included demographic details, premorbid medical conditions and pregnancy, antiviral therapy, and complications associated with influenza. Data on asthma and chronic respiratory disease were collected separately, based on findings from elsewhere which indicated that asthma was a significant risk factor [8,10]. These data were checked by the Departments of Public Health for completeness and cases identified with missing or inconsistent data were followed up and the information corrected. Surveillance and laboratory data were collected on the Irish computerised infectious diseases reporting system (CIDR). The Health Protection Surveillance Centre (HPSC) analysed the data. Analysis of variance (ANOVA) was used to test the effect of age on length of stay.
The prevalence of diseases/risk factors in the population was collected using a variety of methods. Data from the Cystic Fibrosis Registry [12], National Cancer Registry [13] and Infectious Disease Registry [14] were extracted to quantify numbers of people in the population with cystic fibrosis, certain malignancies and acquired immunodeficiency syndrome (AIDS). Hospital In-Patient Enquiry (HIPE) data over four years was used to estimate the prevalence of liver, renal disease and asplenia [15]. The prevalence of haemoglobinopathies was based on personal communication from the clinician with national responsibility for this disease group [16]. The number of pregnant women was extrapolated from the number of births in 2008 [17].
Other estimates were calculated by applying disease prevalence estimates from Irish or international data to the Irish population recorded by the Central Statistics Office (CSO) [17]. Prevalence of asthma and diabetes was estimated extrapolating from prescription data in the Primary Care Re-imbursement Service (PCRS) system (the national scheme providing free medical services to those unable to afford these services without undue hardship; approximately 25% of the population are eligible [18]). Irish and international prevalence studies were used for chronic heart disease [19], respiratory disease [20], obesity [21,22] and neurological disease [23].
Length of stay was calculated as the time from date of admission to date of discharge, or if still in hospital, from date of admission to the date of data extraction from CIDR for analysis (13 October).
Results
During the period from 28 April to 3 October 2009, 205 confirmed cases of pandemic H1N1 influenza were hospitalised, of whom 19 (9.3%) were admitted to ICU.
Of the 205 confirmed hospitalised cases, 106 were female (51.7%). The median age of cases was 21 years (mean age: 25 years; range: five months to 78 years). Seventy-five percent of cases were in persons under 35 years of age (Figure 1).
Figure 1. Cumulative number and age-specific hospitalisation rate for confirmed hospitalised cases, by presence or absence of risk factors, by five-year age groups, Ireland, 28 April ? 3 October 2009 (n=205)

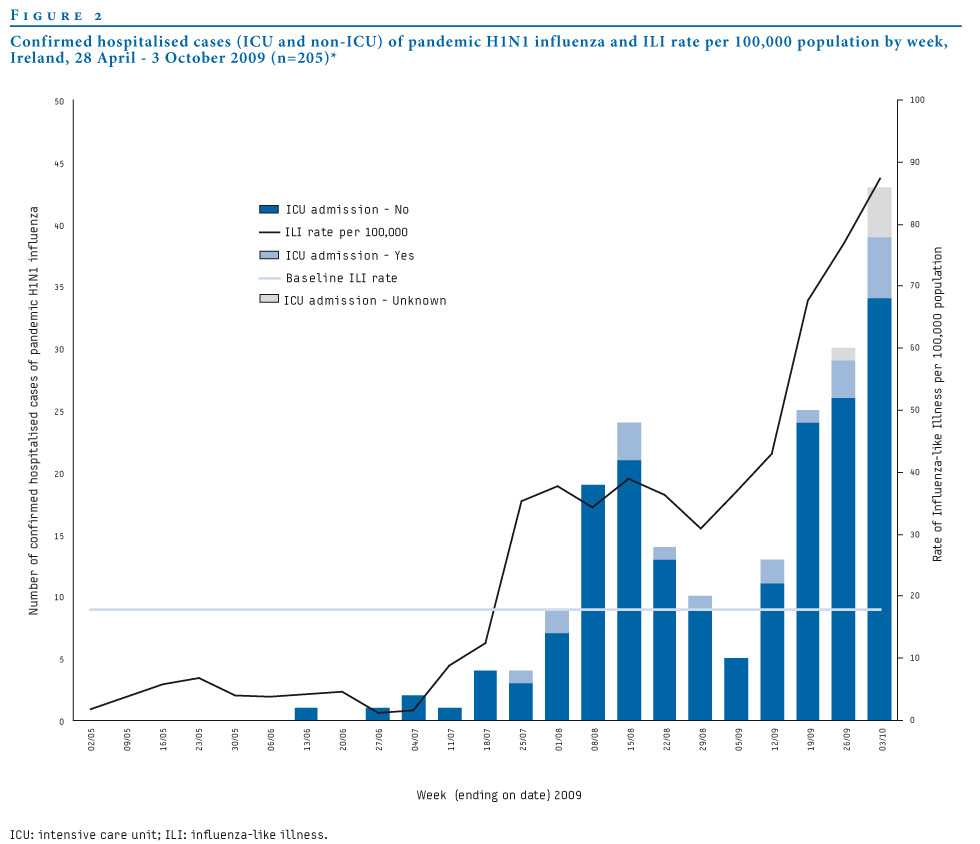
From mid-July there was an increase in the numbers of people hospitalised and admitted to ICU with pandemic H1N1 influenza (Figure 2).
Figure 2. Confirmed hospitalised cases (ICU and non-ICU) of pandemic H1N1 influenza and ILI rate per 100,000 population by week, Ireland, 28 April 3-October 2009 (n=205)

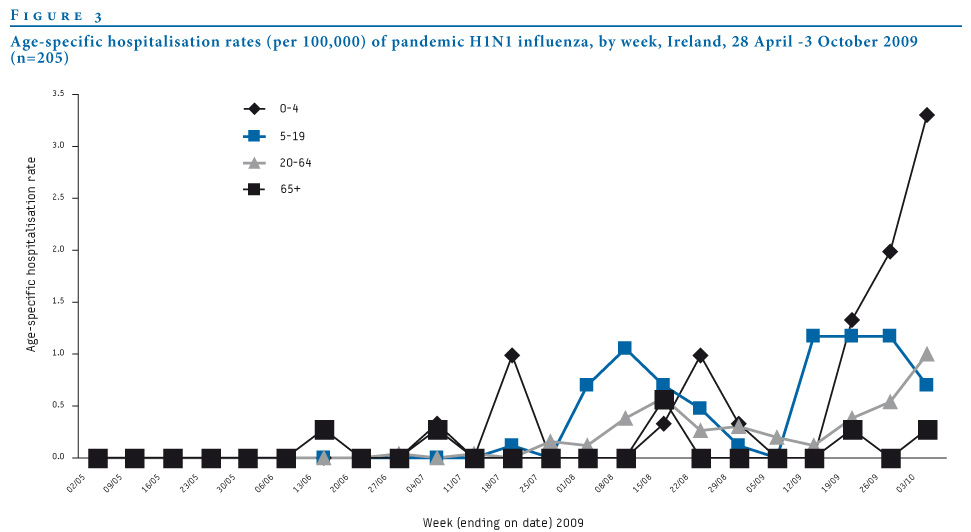
Age-specific hospitalisation rates have been shifting to younger age groups over time, with the highest age-specific rate initially in teenagers and currently in children under five years (age-specific hospitalisation rate <5 years: 3.4/100,000; age-specific hospitalisation rate total population: 1/100,000) (Figure 3).
Figure 3. Age-specific hospitalisation rates (per 100,000) of pandemic H1N1 influenza, by week, Ireland, 28 April -3 October 2009 (n=205)

Information on medical risk factor and pregnancy were available for 180 (88%) of the 205 hospitalised cases including all those admitted to ICU. Ninety-one cases (51%), including eight ICU cases (42%) were not in a recognised risk group.
Eighty-nine cases (49%), including 11 (58%) admitted to ICU, were in a risk group (medical risk factor or pregnancy). Sixty-seven (37%) had only one risk factor, 14 (7%) had two risk factors, seven (4%) had three risk factors and one case had four risk factors.
Twelve pregnant women with pandemic H1N1 influenza were hospitalised, eleven of whom were admitted due to pandemic H1N1 influenza infection, and one was admitted for a pregnancy-related indication. Period of gestation was available for nine women admitted due to influenza; one was in the first trimester, two in the second trimester and six in the third trimester. Three women had risk factors other than pregnancy, including asthma, obesity, liver disease and immunosuppression.
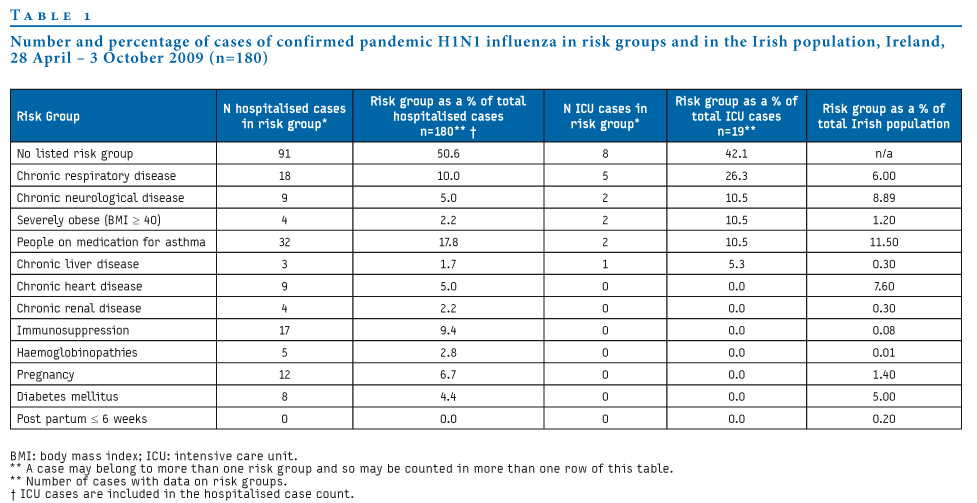
Being on medication for asthma was the most common risk factor for hospitalisation due to pandemic H1N1 influenza. Chronic respiratory disease and immunosuppression were the next most common risk factors. Chronic respiratory disease was the most common risk factor in ICU admissions, followed by chronic neurological disease, asthma and severe obesity (Table 1).
Data on antiviral treatment were available for 196 (96%) of the cases. One hundred and fifty-eight people (79%) received antiviral therapy either prior to admission or in hospital. Oseltamivir was used in 155 people (98%).
Table 1. Number and percentage of cases of confirmed pandemic H1N1 influenza in risk groups and in the Irish population, Ireland, 28 April ? 3 October 2009 (n=180)

Onset date was recorded for 176 (85%) of confirmed cases. Table 2 shows the mean, median and range of the time between date of onset of symptoms and date of diagnosis, date of admission to hospital and date of admission to ICU.
Table 2. Time from onset of symptoms to admission to hospital, to laboratory confirmation, to admission to ICU, and length of stay associated with pandemic H1N1 influenza, Ireland, 28 April - 3 October 2009

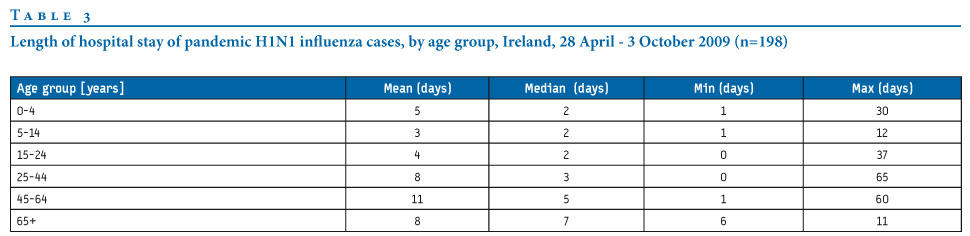
Dates of admission to and discharge from hospital and/or length of stay were recorded for 198 (97%) of cases, including all ICU cases (Table 2). The median length of stay in hospital was two days for cases under the age of 24 years. While there was a large range of length of stay, there was a significant trend of increasing length of stay for those in the age groups of 25-44 year-olds and 45-64 year-olds, increasing to seven days in adults over 65 years (ANOVA: F=3.16, P<0.001) (Table 3).
Table 3. Length of hospital stay of pandemic H1N1 influenza cases, by age group, Ireland, 28 April - 3 October 2009 (n=198)

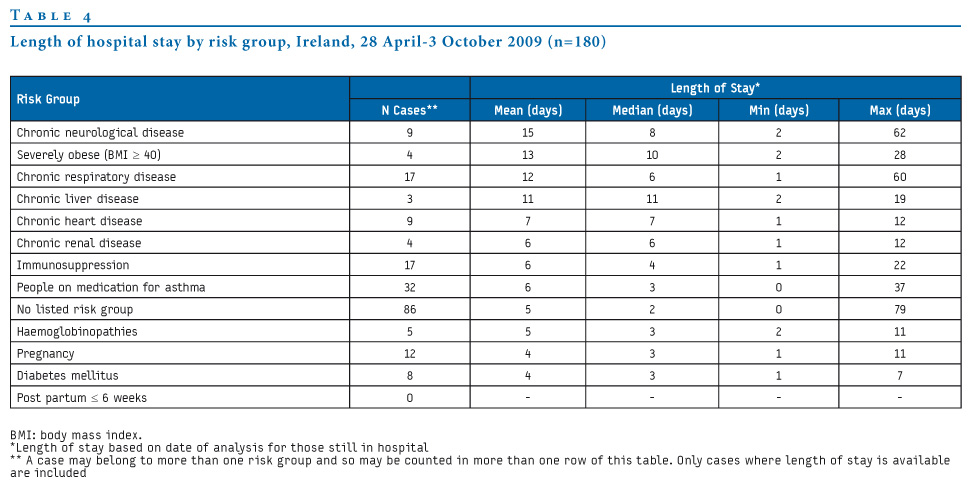
Those with chronic neurological disease had the highest mean length of stay, followed by those with severe obesity and then chronic respiratory disease. Asthma, the most frequent risk factor associated with hospitalisation, was associated with a mean length of stay of six days (median: three days). Most risk-groups were associated with a wide range of length of stay (Table 4).
Table 4. Length of hospital stay by risk group, Ireland, 28 April -3 October 2009 (n=180)

Data on complications were available for 177 (86%) of hospitalised cases. Forty cases (23%) developed pneumonia, 17 (43%) of whom were in a risk group. Ten people (6%) developed adult respiratory distress syndrome (ARDS), of whom six (60%) were in a risk group. Fifteen patients (8%) were ventilated. Fourteen were ventilated in ICU and one received non-invasive ventilation on a general ward.
There were four deaths (2% of hospitalised cases) due to pandemic H1N1 influenza, three females and one male. Two were in the 15-24 year age-group, and two in the 50-59 year age-group. Three fatal cases (75%) had underlying risk factors.
Discussion
The epidemiology of hospitalised cases in the first months of the pandemic was similar in Ireland to other countries [24-28]. While younger age groups were more likely to be hospitalised they had shorter lengths of stay than older age groups. The age specific hospitalisation rate for children in Ireland was lower than that reported elsewhere [27,29,30]. Haemoglobinopathies and immunosuppression were the most over-represented risk factors in hospitalised cases. Pregnancy was associated with an increased risk of hospitalisation with the risk highest in the third trimester. Stay in ICU (median: 22 days; range: 0-72 days) was found to be much longer than reported in other countries [11,27].
The under-representation of children under the age of five years among hospitalised cases when compared with other countries [27,29,30] may be a reflection of the stage of the pandemic wave that Ireland is currently in. It is known that the majority of cases before mid-July were imported [2] and therefore more likely to be in young adults who travel. July and August are school holidays in Ireland and this may have further limited spread among children and thus hospitalisations in children. In this time period the majority of cases in children were associated with residential summer camps [3], suggesting that it is educational settings that are most likely to result in spread in the age groups under 16-year-olds.
The ILI rates exceeded the threshold of seasonal influenza in July, but then reached a plateau in late July and August, and it was only in September (following reopening of schools) that rates started to rise again [3]. International evidence suggests that as the overall number of cases of pandemic H1N1 influenza increases, the age-specific incidence of hospitalisations will shift to younger age groups [10,31]; the same shift is being seen in cases in Ireland. However, in other countries, highest hospitalisation rates were seen in the children under the age of five years at all stages of the pandemic wave, although the magnitude of this difference varied over time [27,31,32].
The under-representation of young children may reflect an ascertainment bias, as children may not present with typical ILI symptoms, and the diagnosis might not have been considered. This has been reported for seasonal influenza [33].
Some patients have an extremely protracted ICU stay, with a number of current patients in ICU in excess of 60 days. There were limited numbers of patients in ICU initially and hence it is difficult to draw conclusions. However, long stays may reflect the availability of suitable step-down facilities, with for instance some smaller acute hospitals having no high dependency units (HDU) to move patients who no longer require full ICU care to. This will impact on ICU and HDU resources as the pandemic progresses.
Length of stay increased with age. One third of children under the age of 15 years had a length of stay of less than two days compared to 25% of the age group of 15-24 year-olds, 17% in the group of 25-64 year-olds and none of the over 65 year-olds. Short lengths of stay in children have been noted elsewhere [8].
Time from onset of symptoms to admission to hospital was shorter than seen in the US [10]. This may be accounted for by the stage of the pandemic in Ireland. Early in the pandemic there was a high level of uncertainty in relation to clinical presentation and likely progression of the disease, which may have led to a lower threshold for early admission to hospital. As clinicians became more experienced in treating pandemic influenza they may have been more confident in advising homecare.
Data gathered in this paper were for surveillance purposes and provide epidemiological information on the early hospitalised cases of pandemic H1N1 influenza. They also provide information on clinical details but it must be borne in mind that the data were not collected primarily for this purpose and so there are a number of limitations. Enhanced surveillance forms were completed at an early stage of hospitalisation and were updated where possible later during the stay and at discharge. A retrospective chart review was not carried out. This may impact on data validity, particularly recording of influenza complications and on time of onset of symptoms. Data on risk factors were gathered from the treating clinician and may have been subject to bias such as misclassification bias. The proportion of hospitalised cases with risk factors was lower than that reported in studies elsewhere. This may be due to the fact that a detailed case review of each patient?s notes was not carried out, as was done elsewhere [10,11]. However, efforts were made to ensure that data collected from clinicians was complete, and incomplete data was rechecked at a later stage, with over 90% of data completed. Also, as data were collected on all hospitalised cases in Ireland, there was less potential for bias than would have occurred if the cases were a sample presenting at one or a few sites.
The prevalence of risk groups in the general population were derived by a number of different methods based on data of varying quality. Information on pregnancy and diseases for which registries are available can be considered reliable. Other data are of varying quality and should be interpreted with caution. Nevertheless, they provide some indication of the representation of different risk groups among hospitalised cases compared with their distribution within the general population as well as some indication as to whether they are over- or underrepresented.
Surveillance data continue to be very important in understanding the pandemic in Ireland. However, information needs have changed. It is now important to identify those at highest risk of complications and to understand what those complications are in order to plan both prevention strategies and hospital surge capacity. Hospital surveillance will continue to be important. In addition, enhanced surveillance of ICU cases has been implemented in Ireland and will provide more information on complications in these patients, particularly severe complications.
Acknowledgements:
A vast number of people from the National Public Health Outbreak Response Team, which includes the Departments of Public Health, the National Virus Reference Laboratory, the Health Protection Surveillance Centre, the Assistant National Director- Health Protection, as well as hospital clinicians have contributed to the data collected here.
<hr>References
<hr>
Eurosurveillance, Volume 14, Issue 44, 05 November 2009
Rapid communications
Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April ? 3 October 2009
G Cullen<sup>1</sup>, J Martin (
- Health Protection Surveillance Centre, Dublin, Ireland
- Department of Public Health HSE East, Ireland
- Department of Public Health, HSE West, Ireland
- Department of Public Health, HSE South, Ireland
- Department of Public Health, HSE Dublin, Mid Leinster, Ireland
<hr> Citation style for this article: Cullen G, Martin J, O?Donnell J, Boland M, Canny M, Keane E, McNamara A, O?Hora A, Fitzgerald M, Jackson S, Igoe D, O?Flanagan D. Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April ? 3 October 2009. Euro Surveill. 2009;14(44):pii=19389. Available online: LINK
Date of submission: 19 October 2009
<hr> From 28 April 2009 to 3 October 2009, 205 cases of confirmed pandemic H1N1 influenza were hospitalised in Ireland. Detailed case-based epidemiological information was gathered on all hospitalised cases. Age-specific hospitalisation rates were highest in the age group of 15 to 19 year-olds and lowest in those aged 65 years and over. Nineteen hospitalised cases (9%) were admitted to intensive care units (ICU) where the median length of stay was 24 days. Four hospitalised cases (2%) died. Fifty-one percent of hospitalised cases and 42% of ICU cases were not in a recognised risk group. Asthma was the most common risk factor among cases; however, people with haemoglobinopathies and immunosuppression were the most over-represented groups.
<hr>Introduction In late April 2009, a novel influenza virus led to human infection in Mexico and the United States (US) and subsequently spread worldwide. On 11 June, 2009, the World Health Organization (WHO) declared a phase 6 pandemic of moderate severity [1].
The first case of pandemic influenza in Ireland was diagnosed on 28 April 2009. Existing surveillance systems were augmented and enhanced case-based surveillance of pandemic H1N1 influenza was commenced. Until mid-July, all cases of influenza were actively followed up; most cases were imported, mainly from the US, the majority were in young adults and there were few hospitalisations [2]. On 16 July Ireland moved to mitigation, and detailed case-based surveillance was confined to hospitalised cases. Influenza-like illness (ILI) presentations to sentinel general practices remained below the seasonal threshold (17.8/100,000) between April and mid-July [3]. By late July, the ILI rate reached 35 per 100,000 population and fluctuated around this level until mid-September. Since then ILI rates have risen, reaching 87.3 per 100,000 population in the week ending 3 October [3].
The WHO has recommended that countries undertake case-based surveillance on the first 200 hospitalised cases, as it is important to identify those most at risk of adverse outcomes, hospitalisation and death due to pandemic H1N1 influenza. To date, there is limited research on risk factors associated with adverse outcomes in Europe [4-11] and therefore, we report on the enhanced case-based surveillance of the first 205 hospitalised cases of confirmed pandemic H1N1 influenza in Ireland.
Methods
Enhanced surveillance was undertaken on all cases of confirmed pandemic H1N1 influenza deemed to require admission to hospital for management of their illness by the treating clinician. Regional Departments of Public Health or the treating hospital clinician completed the enhanced surveillance form. Data collected included demographic details, premorbid medical conditions and pregnancy, antiviral therapy, and complications associated with influenza. Data on asthma and chronic respiratory disease were collected separately, based on findings from elsewhere which indicated that asthma was a significant risk factor [8,10]. These data were checked by the Departments of Public Health for completeness and cases identified with missing or inconsistent data were followed up and the information corrected. Surveillance and laboratory data were collected on the Irish computerised infectious diseases reporting system (CIDR). The Health Protection Surveillance Centre (HPSC) analysed the data. Analysis of variance (ANOVA) was used to test the effect of age on length of stay.
The prevalence of diseases/risk factors in the population was collected using a variety of methods. Data from the Cystic Fibrosis Registry [12], National Cancer Registry [13] and Infectious Disease Registry [14] were extracted to quantify numbers of people in the population with cystic fibrosis, certain malignancies and acquired immunodeficiency syndrome (AIDS). Hospital In-Patient Enquiry (HIPE) data over four years was used to estimate the prevalence of liver, renal disease and asplenia [15]. The prevalence of haemoglobinopathies was based on personal communication from the clinician with national responsibility for this disease group [16]. The number of pregnant women was extrapolated from the number of births in 2008 [17].
Other estimates were calculated by applying disease prevalence estimates from Irish or international data to the Irish population recorded by the Central Statistics Office (CSO) [17]. Prevalence of asthma and diabetes was estimated extrapolating from prescription data in the Primary Care Re-imbursement Service (PCRS) system (the national scheme providing free medical services to those unable to afford these services without undue hardship; approximately 25% of the population are eligible [18]). Irish and international prevalence studies were used for chronic heart disease [19], respiratory disease [20], obesity [21,22] and neurological disease [23].
Length of stay was calculated as the time from date of admission to date of discharge, or if still in hospital, from date of admission to the date of data extraction from CIDR for analysis (13 October).
Results
During the period from 28 April to 3 October 2009, 205 confirmed cases of pandemic H1N1 influenza were hospitalised, of whom 19 (9.3%) were admitted to ICU.
Of the 205 confirmed hospitalised cases, 106 were female (51.7%). The median age of cases was 21 years (mean age: 25 years; range: five months to 78 years). Seventy-five percent of cases were in persons under 35 years of age (Figure 1).
Figure 1. Cumulative number and age-specific hospitalisation rate for confirmed hospitalised cases, by presence or absence of risk factors, by five-year age groups, Ireland, 28 April ? 3 October 2009 (n=205)

From mid-July there was an increase in the numbers of people hospitalised and admitted to ICU with pandemic H1N1 influenza (Figure 2).
Figure 2. Confirmed hospitalised cases (ICU and non-ICU) of pandemic H1N1 influenza and ILI rate per 100,000 population by week, Ireland, 28 April 3-October 2009 (n=205)
Age-specific hospitalisation rates have been shifting to younger age groups over time, with the highest age-specific rate initially in teenagers and currently in children under five years (age-specific hospitalisation rate <5 years: 3.4/100,000; age-specific hospitalisation rate total population: 1/100,000) (Figure 3).
Figure 3. Age-specific hospitalisation rates (per 100,000) of pandemic H1N1 influenza, by week, Ireland, 28 April -3 October 2009 (n=205)
Information on medical risk factor and pregnancy were available for 180 (88%) of the 205 hospitalised cases including all those admitted to ICU. Ninety-one cases (51%), including eight ICU cases (42%) were not in a recognised risk group.
Eighty-nine cases (49%), including 11 (58%) admitted to ICU, were in a risk group (medical risk factor or pregnancy). Sixty-seven (37%) had only one risk factor, 14 (7%) had two risk factors, seven (4%) had three risk factors and one case had four risk factors.
Twelve pregnant women with pandemic H1N1 influenza were hospitalised, eleven of whom were admitted due to pandemic H1N1 influenza infection, and one was admitted for a pregnancy-related indication. Period of gestation was available for nine women admitted due to influenza; one was in the first trimester, two in the second trimester and six in the third trimester. Three women had risk factors other than pregnancy, including asthma, obesity, liver disease and immunosuppression.
Being on medication for asthma was the most common risk factor for hospitalisation due to pandemic H1N1 influenza. Chronic respiratory disease and immunosuppression were the next most common risk factors. Chronic respiratory disease was the most common risk factor in ICU admissions, followed by chronic neurological disease, asthma and severe obesity (Table 1).
Data on antiviral treatment were available for 196 (96%) of the cases. One hundred and fifty-eight people (79%) received antiviral therapy either prior to admission or in hospital. Oseltamivir was used in 155 people (98%).
Table 1. Number and percentage of cases of confirmed pandemic H1N1 influenza in risk groups and in the Irish population, Ireland, 28 April ? 3 October 2009 (n=180)
Onset date was recorded for 176 (85%) of confirmed cases. Table 2 shows the mean, median and range of the time between date of onset of symptoms and date of diagnosis, date of admission to hospital and date of admission to ICU.
Table 2. Time from onset of symptoms to admission to hospital, to laboratory confirmation, to admission to ICU, and length of stay associated with pandemic H1N1 influenza, Ireland, 28 April - 3 October 2009

Dates of admission to and discharge from hospital and/or length of stay were recorded for 198 (97%) of cases, including all ICU cases (Table 2). The median length of stay in hospital was two days for cases under the age of 24 years. While there was a large range of length of stay, there was a significant trend of increasing length of stay for those in the age groups of 25-44 year-olds and 45-64 year-olds, increasing to seven days in adults over 65 years (ANOVA: F=3.16, P<0.001) (Table 3).
Table 3. Length of hospital stay of pandemic H1N1 influenza cases, by age group, Ireland, 28 April - 3 October 2009 (n=198)
Those with chronic neurological disease had the highest mean length of stay, followed by those with severe obesity and then chronic respiratory disease. Asthma, the most frequent risk factor associated with hospitalisation, was associated with a mean length of stay of six days (median: three days). Most risk-groups were associated with a wide range of length of stay (Table 4).
Table 4. Length of hospital stay by risk group, Ireland, 28 April -3 October 2009 (n=180)
Data on complications were available for 177 (86%) of hospitalised cases. Forty cases (23%) developed pneumonia, 17 (43%) of whom were in a risk group. Ten people (6%) developed adult respiratory distress syndrome (ARDS), of whom six (60%) were in a risk group. Fifteen patients (8%) were ventilated. Fourteen were ventilated in ICU and one received non-invasive ventilation on a general ward.
There were four deaths (2% of hospitalised cases) due to pandemic H1N1 influenza, three females and one male. Two were in the 15-24 year age-group, and two in the 50-59 year age-group. Three fatal cases (75%) had underlying risk factors.
Discussion
The epidemiology of hospitalised cases in the first months of the pandemic was similar in Ireland to other countries [24-28]. While younger age groups were more likely to be hospitalised they had shorter lengths of stay than older age groups. The age specific hospitalisation rate for children in Ireland was lower than that reported elsewhere [27,29,30]. Haemoglobinopathies and immunosuppression were the most over-represented risk factors in hospitalised cases. Pregnancy was associated with an increased risk of hospitalisation with the risk highest in the third trimester. Stay in ICU (median: 22 days; range: 0-72 days) was found to be much longer than reported in other countries [11,27].
The under-representation of children under the age of five years among hospitalised cases when compared with other countries [27,29,30] may be a reflection of the stage of the pandemic wave that Ireland is currently in. It is known that the majority of cases before mid-July were imported [2] and therefore more likely to be in young adults who travel. July and August are school holidays in Ireland and this may have further limited spread among children and thus hospitalisations in children. In this time period the majority of cases in children were associated with residential summer camps [3], suggesting that it is educational settings that are most likely to result in spread in the age groups under 16-year-olds.
The ILI rates exceeded the threshold of seasonal influenza in July, but then reached a plateau in late July and August, and it was only in September (following reopening of schools) that rates started to rise again [3]. International evidence suggests that as the overall number of cases of pandemic H1N1 influenza increases, the age-specific incidence of hospitalisations will shift to younger age groups [10,31]; the same shift is being seen in cases in Ireland. However, in other countries, highest hospitalisation rates were seen in the children under the age of five years at all stages of the pandemic wave, although the magnitude of this difference varied over time [27,31,32].
The under-representation of young children may reflect an ascertainment bias, as children may not present with typical ILI symptoms, and the diagnosis might not have been considered. This has been reported for seasonal influenza [33].
Some patients have an extremely protracted ICU stay, with a number of current patients in ICU in excess of 60 days. There were limited numbers of patients in ICU initially and hence it is difficult to draw conclusions. However, long stays may reflect the availability of suitable step-down facilities, with for instance some smaller acute hospitals having no high dependency units (HDU) to move patients who no longer require full ICU care to. This will impact on ICU and HDU resources as the pandemic progresses.
Length of stay increased with age. One third of children under the age of 15 years had a length of stay of less than two days compared to 25% of the age group of 15-24 year-olds, 17% in the group of 25-64 year-olds and none of the over 65 year-olds. Short lengths of stay in children have been noted elsewhere [8].
Time from onset of symptoms to admission to hospital was shorter than seen in the US [10]. This may be accounted for by the stage of the pandemic in Ireland. Early in the pandemic there was a high level of uncertainty in relation to clinical presentation and likely progression of the disease, which may have led to a lower threshold for early admission to hospital. As clinicians became more experienced in treating pandemic influenza they may have been more confident in advising homecare.
Data gathered in this paper were for surveillance purposes and provide epidemiological information on the early hospitalised cases of pandemic H1N1 influenza. They also provide information on clinical details but it must be borne in mind that the data were not collected primarily for this purpose and so there are a number of limitations. Enhanced surveillance forms were completed at an early stage of hospitalisation and were updated where possible later during the stay and at discharge. A retrospective chart review was not carried out. This may impact on data validity, particularly recording of influenza complications and on time of onset of symptoms. Data on risk factors were gathered from the treating clinician and may have been subject to bias such as misclassification bias. The proportion of hospitalised cases with risk factors was lower than that reported in studies elsewhere. This may be due to the fact that a detailed case review of each patient?s notes was not carried out, as was done elsewhere [10,11]. However, efforts were made to ensure that data collected from clinicians was complete, and incomplete data was rechecked at a later stage, with over 90% of data completed. Also, as data were collected on all hospitalised cases in Ireland, there was less potential for bias than would have occurred if the cases were a sample presenting at one or a few sites.
The prevalence of risk groups in the general population were derived by a number of different methods based on data of varying quality. Information on pregnancy and diseases for which registries are available can be considered reliable. Other data are of varying quality and should be interpreted with caution. Nevertheless, they provide some indication of the representation of different risk groups among hospitalised cases compared with their distribution within the general population as well as some indication as to whether they are over- or underrepresented.
Surveillance data continue to be very important in understanding the pandemic in Ireland. However, information needs have changed. It is now important to identify those at highest risk of complications and to understand what those complications are in order to plan both prevention strategies and hospital surge capacity. Hospital surveillance will continue to be important. In addition, enhanced surveillance of ICU cases has been implemented in Ireland and will provide more information on complications in these patients, particularly severe complications.
Acknowledgements:
A vast number of people from the National Public Health Outbreak Response Team, which includes the Departments of Public Health, the National Virus Reference Laboratory, the Health Protection Surveillance Centre, the Assistant National Director- Health Protection, as well as hospital clinicians have contributed to the data collected here.
<hr>References
- World Health Organization. Influenza A (H1N1): WHO announces pandemic alert phase 6, of moderate severity. Copenhagen:WHO;2009. Available from: http://www.euro.who.int/mediacentre/PR/2009/20090611_1
- Martin J, O'Donnell J, Igoe D, O'Hora A, Thornton L, Murphy N, et al. Enhanced surveillance of initial cases of pandemic H1N1 2009 influenza in Ireland, April - July 2009 . Euro Surveill 2009;14(38). pii=19337. Available from: http://www.eurosurveillance.org/View...rticleId=19337
- Health Protection Surveillance Centre. Influenza Surveillance in Ireland - Weekly Update Influenza Week 41 2009. 2009. Available from: http://www.hpsc.ie/hpsc/A-Z/Emergenc...nce%20Reports/
- Jamieson DJ, Honien MA, Rasmussen SA. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374(9688):451-8.
- Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team, Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, Garten RJ, et al. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360(25):2605-15. Available from: http://content.nejm.org/cgi/content/...EJMoa0903810v3
- Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Qui?ones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 2009;36:680-9.
- Vaillant L, La Ruche G, Tarantola A, Barboza P; epidemic intelligence team at InVS. Epidemiology of fatal cases associated with pandemic H1N1 influenza 2009. Euro Surveill 2009;14(33). pii: 19309. Available from: http://www.eurosurveillance.org/View...rticleId=19309
- Hacket S, Hill L, Patel J, Ratnaraja N, Ifeyinwa A, Farooqi M, et al. Clinical characteristics of paediatric H1N1 admissions in Birmingham, UK. Lancet 2009;374(9690):605. Available from: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(09)61511-7/fulltext?version=printerFriendly
- Raffo L. [Influenza A(H1N1) epidemic in Argentina. Experience in a National General Hospital (Hospital Nacional Alejandro Posadas)]. Medicina (B Aires). 2009;69(4):393-423. [Article in Spanish]
- Jain S, Kamimoto L, Bramley A, Schmitz A, Benoit S, Louie J, et al. Hospitalized Patients with 2009 H1N1 Influenza in the United States, April-June 2009. N Engl J Med 2009. Available from: http://content.nejm.org/cgi/reprint/NEJMoa0906695v1.pdf
- The Anzic Influenza Investigators. Critical Care Services and 2009 H1N1 Influenza in Australia and New Zealand. N Engl J Med. 2009. Available from: http://content.nejm.org/cgi/reprint/NEJMoa0908481v1.pdf
- The Cystic Fibrosis Registry of Ireland. CF annual report 2007. 2007. Available from: http://www.cfri.ie/docs/annual_repor...7_registry.pdf
- National Cancer Registry Ireland. Cancer in Ireland 1994-2005 a summary. 2006. Available from: http://www.ncri.ie/pubs/pubfiles/summary2007.pdf
- Health Protection Surveillance Centre. HPSC, Annual Report 2007. 2008. Available from: http://www.hpsc.ie/hpsc/AboutHPSC/An...le,3377,en.pdf
- O'Loughlin R, Allwright S, Barry J, Kelly A, Teljeur C. Using HIPE data as a research and planning tool: limitations and opportunities. Ir J Med Sci. 2005;174(4):66.
- Corrina McMahon, Our Lady's Children's Hospital C. 2009.
- Central Statistics Office. Vital Statistics, Fourth Quarter and Yearly Summary, 2008. 2009. Available from: http://www.cso.ie/releasespublicatio...ent/vstats.pdf
- Health Service Executive. Primary Care Re-imbursement Service. 2009. Available from: http://www.citizensinformation.ie/ca...payments_board
- Creagh D, Neilson S, Collins A, Colwell N, Hinchion R, Drew C, et al. Established cardiovascular disease and CVD risk factors in a primary care population of middle-aged Irish men and women. Ir Med J. 2002 Nov;95(10):298-301.
- Schirnhofer L, Lamprecht B, Vollmer WM, Allison MJ, Studnicka M, Jensen RL, et al. COPD prevalence in Salzburg, Austria: results from the Burden of Obstructive Lung Disease (BOLD) Study. Chest. 2007;131(1):29-36.
- Whelton H, Harrington J, Crowley E, Kelleher V, Cronin M, Perry IJ. Prevalence of overweight and obesity on the island of Ireland: results from the North South Survey of Children's Height, Weight and Body Mass Index, 2002. BMC Public Health. 2007;7:187.
- Institute of Public Health in Ireland. Making diabetes count - what does the future hold? A systematic approach to forecasting population prevalence on the island of Ireland in 2010 and 2015. 2006 Jan 4. Available from: http://www.publichealth.ie/files/fil...ure%20hold.pdf
- The neurological alliance. Neuro numbers: a brief review of the numbers of people in the UK with a neurological condition. 2003. Available from: http://www.neural.org.uk/store/asset...uroNumbers.pdf
- Gilsdorf A, Poggensee G, on behalf of the working group pandemic influenza A (H1N1)v. Description of the early stage of pandemic (H1N1) 2009 in Germany, 27 April-16 June 2009. Euro Surveill 2009;14(31). pii:19295. Available from: http://www.eurosurveillance.org/View...rticleId=19295
- Belgian working group on influenza A(H1N1)v. Influenza A(H1N1)v virus infections in Belgium, May-June 2009. Euro Surveill 2009;14(28). pii: 19270. Available from: http://www.eurosurveillance.org/View...rticleId=19270
- ECDC Technical Emergency Team. Initial epidemiological findings in the European Union following the declaration of pandemic alert level 5 due to influenza A (H1N1). Euro Surveill 2009;14(18). pii: 19204. Available from: http://www.eurosurveillance.org/View...rticleId=19204
- Australian Government Department of Health and Ageing. Australian Influenza Surveillance Summary Report No. 19. 2009. Available from: http://www.healthemergency.gov.au/in...-no19-2009.pdf
- Finelli L, Brammer L, Blanton L, Epperson S, Dhara R, Fowlkes A, et al. Update: Influenza Activity --- United States, April--August 2009. 2009 Sep 10. Available from: http://www.cdc.gov/mmwr/preview/mmwr...=mm58e0910a1_x
- Baker MG, Wilson N, Huang QS, Paine S, Lopez L, Bandaranayake D, et al. Pandemic influenza A(H1N1)v in New Zealand: the experience from April to August 2009. Euro Surveill 2009;14(34). pii: 19319. Available from: http://www.eurosurveillance.org/View...rticleId=19319
- Health Protection Agency. HPA Weekly National Influenza Report 24 September 2009 (Week 39). 2009. Available from: http://www.hpa.nhs.uk/web/HPAwebFile.../1253205412438
- Health Protection Agency. Situation Report of the Influenza Pandemic (H1N1) 2009 (Swine Flu) in the United Kingdom, no.81 Oct 14 2009. 2009.
- Australian Government Department of Health and Ageing. Australian Influenza Surveillance Summary Report No.17. 2009. Available from: http://www.healthemergency.gov.au/in...-no17-2009.pdf
- Poehling KA, Edwards KM, Weinberg GA, Szilagyi P, Staat MA, Iwane MK, et al. The underrecognized burden of influenza in young children. N Engl J Med. 2006;355(1):31-40.
<hr>