-
SARS CoV-2 Viral Persistence Study (PASC) - Study of Long COVID-19 (PASC)
Drug: Paxlovid
Study Description
Brief Summary:
This study is a platform protocol designed to be flexible so that it is suitable for a wide range of settings within health care systems and in community settings where it can be integrated into COVID-19 programs and subsequent treatment plans.
This protocol is a prospective, multi-center, multi-arm, double-blind, randomized, controlled platform trial evaluating antiviral and other therapeutics for use in the treatment of Post-Acute Sequelae of COVID-19 (PASC). The hypothesis is that persistent viral infection (antigenemia) and/or overactive/chronic immune response (inflammation) are underlying contributors to PASC and that antiviral and other applicable therapies may result in viral clearance or decreased inflammation and improvement in PASC symptoms.
-

Pinned Tweet

Bunk the Biologist
@BiologistBunk
PhD in Immunology, Cell Biologist. Two-time covid long hauler. Admin of the FB group Long Covid - recover via Fasting /Autophagy Lactobacillus for Long Covid
Boulder, CO recoverfromlongcovid.com/?p=517Joined November 2020
Bunk the Biologist
@BiologistBunk
Jul 11
I have updated my characterization of Long Covid and my comparison of #vaccineinjured and #LongCovid symptoms. The pattern of symptoms and median severities are nearly identical. I propose that both can be explained by low-level viral infection. https://recoverfromlongcovid.com/?page_id=413
Leave a comment:
-
Sharon, the first post promoted vaccines in relation to LC. I think people should know that people are getting LC even when fully vaxxed and boosted and when they have access to Paxlovid. They don't get better in the long run by getting another booster to try to fix it from what I read. If the chair of medicine at UCSF is not relevant, credible and useful sharing his wife's experience, what is?
-
I moved two posts off this thread because they were off topic. Vaccines and covid drugs are not the focus on this thread.
Long covid is real and is most probably caused by the immune system's over-reaction to the illness. Apparently this over-reaction can cause tiny micro filament clots that the body does not have the natural process to break down:
@RajeevJayadevan
UK Cardiologist Rae Duncan explains Long COVID beautifully. Abnormal, prolonged immune response damages the inner lining of blood vessels. Micro clots form, of abnormal molecular structure, that the body’s usual mechanisms can’t get rid of. They show up in various organs.
Start at 31:02
Leave a comment:
-
-
David Fisman
@DFisman
·
39m
Diseases that affect small blood vessels, like lupus and syphilis, are often referred to as “great imitators”, because their manifestations are protean…you have small blood vessels everywhere.
You can reply to this conversation
1
22
88
David Fisman
@DFisman
·
21m
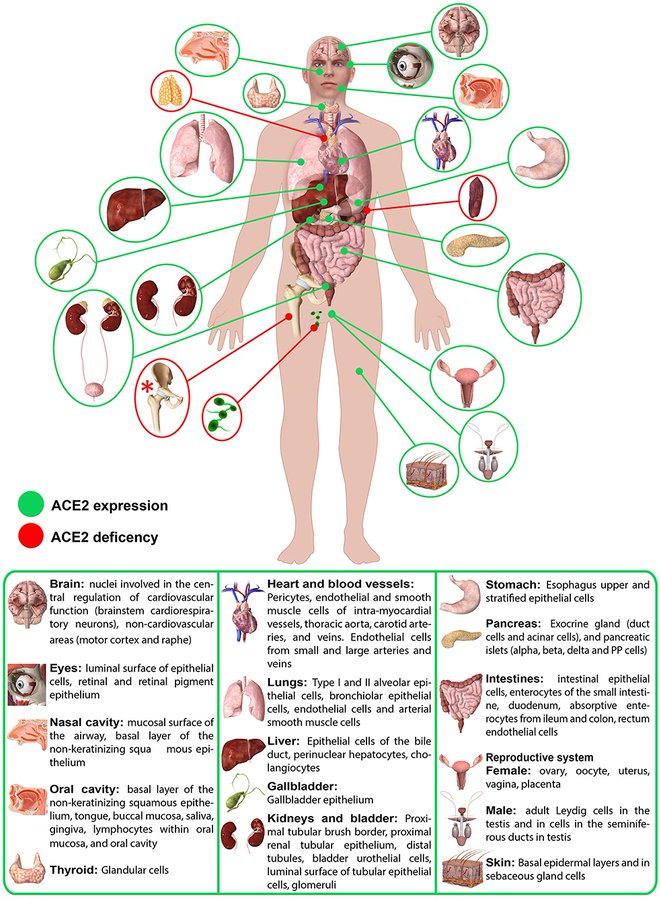
Sars-2 latches onto a chemical called ace-2, which is ubiquitous in “epithelial” cells (cells that line your respiratory tract) but also “endothelial” cells (cells that line your blood vessels, and have important functions, like helping regulate blood pressure).
1
24
41
David Fisman
@DFisman
·
16m
It’s unsurprising then that sars-2 is starting to emerge as a great imitator in its own right. The virus was initially regarded as a dominantly respiratory pathogen, like RSV. But it’s becoming clear that it’s much more than that.Leave a comment:
-
Well apparently 45% of US households (which averages three individuals) is stressed out about $$$ alone. No mention of covid needed:
Inflation Causing Hardship for 45% of U.S. Households
This would mean, according to the paper above, that a large percentage of the population is susceptible to long covid.Leave a comment:
-
https://www.nichd.nih.gov/newsroom/n...gical-distress
Science Update: Pre-existing distress may increase risk for long COVID, NIH-funded study suggests
Friday, September 23, 2022
Psychological distress before COVID-19 infection—feeling stressed, depressed, anxious, worried, or lonely—may raise the risk for long COVID, suggests a study funded by the National Institutes of Health. Long COVID includes such symptoms as fatigue, brain fog, breathing difficulties, and other symptoms that may persist for months after a COVID-19 infection.
The researchers cautioned that their findings should not be misinterpreted to support the view that long COVID symptoms are psychosomatic. Among study participants who developed long COVID, almost half had no psychological distress before COVID-19 infection. Many symptoms of long COVID, such as breathing difficulties and loss of taste and smell, are not common symptoms of mental illness. The authors called for more research to determine if alleviating psychological distress before COVID-19 infection reduces the chances or severity of long COVID.
The study was conducted by Siwen Wang, M.D., of the Harvard T.H. Chan School of Medicine, and colleagues. It appears in JAMA Psychiatry. The study was funded by NIH’s Eunice Kennedy Shriver National Institute of Child Health and Human Development; National Heart, Lung, and Blood Institute; National Institute of Environmental Health Sciences; and National Cancer Institute.
Background
Long COVID involves a wide range of symptoms that last more than four weeks and sometimes for many months after a COVID-19 infection. Symptoms, such as fatigue, breathing difficulty, shortness of breath, brain fog (difficulty thinking or concentrating), and loss of taste and smell, may also go away and come back again. Risk factors for long COVID include older age, obesity, severe COVID-19 infection, high blood pressure, depressed immune system, and asthma.
The researchers analyzed data from three long-term studies, two of which enrolled nurses and a another which enrolled children of nurses. From April 2020 to September 2020, participants, almost 97% female, responded to a baseline questionnaire on whether they were experiencing psychological distress, such as depression, anxiety, worry about COVID-19, stress, and loneliness. After the baseline questionnaire, nearly 55,000 participants responded to monthly questionnaires until November 2021 on their overall health.
Results
During the 19 months after the baseline questionnaire, 6% (3,193 participants) tested positive for COVID-19, with 1,403 long COVID cases.
Long COVID was 32% more likely among those who had symptoms of depression, 42% more likely among those with symptoms of anxiety, 37% more likely among those who were worried about COVID-19, 46% more likely among those who felt stressed, and 32% more likely among those who felt lonely. Participants who reported two or more types of distress were almost 50% more likely to develop long COVID.
Significance
The authors concluded that psychological distress before COVID-19 infection may be a risk factor for long COVID. They noted that psychological distress is linked to inflammation and may also suppress the immune system, factors which they theorized could increase the risk for long COVID symptoms.
“We need to consider psychological health in addition to physical health as risk factors of long COVID,” said the study’s senior author, Andrea Roberts, Ph.D., M.P.H., of the Harvard T.H. Chan School of Medicine.
Reference
Wang, S, et al. Associations of depression, anxiety, worry, perceived stress, and loneliness prior to infection with risk of post-COVID-19 conditions. JAMA Psychiatry. 2022. doi: 10.1001/jamapsychiatry.2022.2640
Content OwnerOffice of Communications Last Reviewed Date9/23/2022Leave a comment:
-
She did not say that everyone should be "afraid". That is your word. -
Unintentionally, I'm sure, but she sounds like another vaccine commercial.
Everyone should be afraid? I read there are risk factors for the diagnosis: female, overweight, pre-existing anxiety. The anxiety is a big one so when media/researchers/government increase anxiety to promote vaccines, they are creating more 'long Covid.'"Who I've seen.... Humans of all ages. 21 through 87. All demographics. Previously healthy. Previously not healthy. Teachers and healthcare workers. So many teachers and healthcare workers. Athletes. Non athletes. It's non-discrimnatory."
2020 was back when original strains were circulating. Even including that time period leaves the evidence 'weak' as far as protection.2. Vax vs unvaxxed - remember, this is a small sample size. Purely anecdotal. Those that got COVID in 2020 prior to vaccine being available (in my cohort) show far more debilitating and severe long COVID than those with even one dose. Vaccinated individuals can still get LC.
Leave a comment:
-
Discussion - Long COVID
Neeja Bakshi
@NeejaB
A very long - Long COVID thread. Our Long COVID program has been open 10 months now. I've seen over 150 patients in that time, with new referrals booking well into February 2023.
10:56 PM · Oct 27, 2022·Twitter for Android
1,564
Retweets
159
Quote Tweets
4,486
Likes

Tweet your reply
Reply
Neeja Bakshi
@NeejaB
·
13h
Replying to
@NeejaB
I've had to stop accepting other internal medicine referrals, just so I can keep up with the demand, the follow ups, the downstream effect.
3
39
638
Neeja Bakshi
@NeejaB
·
13h
What I've learned... There are definite patterns. Dysautonomia/POTS. Cognitive dysfunction and brain fog. PEM (post exertional malaise). Unexplained rashes. Muscles feeling like cement. Migraines. Chest pain. So much chest pain. Shortness of breath.
16
195
1,265
Neeja Bakshi
@NeejaB
·
13h
Who I've seen.... Humans of all ages. 21 through 87. All demographics. Previously healthy. Previously not healthy. Teachers and healthcare workers. So many teachers and healthcare workers. Athletes. Non athletes. It's non-discrimnatory.
3
160
1,242
Neeja Bakshi
@NeejaB
·
13h
How my clinical process has evolved.... Pre-appt screening tests, quality of life scores, functional assessment scores. During appointment visual aids to help understand possible pathophysiology.
2
33
645
Neeja Bakshi
@NeejaB
·
13h
Comprehensive educational documentation with personalized recommendations for each patient as info is often overwhelming, esp with brain fog. Treatment aimed at both "Band-Aid toolbox" to help quality of life and "Root cause" looking at immunomodulation, anti-inflammation.
3
45
724
Neeja Bakshi
@NeejaB
·
13h
Nursing and physician check ins. Regularly. Reflective listening, validation, and commiseration. Continuously reading, searching, hoping to find next breakthrough or tool that can be used.
3
35
676
Neeja Bakshi
@NeejaB
·
13h
Barriers I've discovered - insurance. Insurance. Insurance. Insurance. Pages and pages of forms, minimizing my judgement, experience and clinical knowledge.
4
139140
1,251
Neeja Bakshi
@NeejaB
·
13h
Neeja Bakshi
@NeejaB
·
13h
Fighting tooth and nail to have claim adjusters understand that "pushing through" and excessive functional assessments for the patient is contraindicated in patients with long COVID and ME/CFS.
2
126
1,120
Neeja Bakshi
@NeejaB
·
13h
And through all of this, trying to manage my own long COVID experience. Which has required pacing, reinvention of my chart note template to help cue the next question I was supposed to ask.
1
40
897
Neeja Bakshi
@NeejaB
·
13h
I let my patients know at the beginning of their long covid assessment, that the 90 minutes allotted is not only for them, but for me... As I will undoubtedly require the time and space to fully stay on task.
1
36
806
Neeja Bakshi
@NeejaB
·
12h
The 15 minute buffers I have to place throughout my day to regain the line of questioning and follow through needed that comes with each individual's Long COVID story.
2
28
671
Neeja Bakshi
@NeejaB
·
12h
10 months in, some of my patients have been able to be discharged, feeling almost close to pre -COVID health. Some have gotten COVID again, which worsens their symptoms and we start everything from scratch.
3
78
820
Neeja Bakshi
@NeejaB
·
13h
But the vast majority of Long COVID patients are in this purgatory. Not knowing which way their life is going to go. Is this the best it's going to be? Am I one illness away from going back to where I started? Will I be able to work again? Will I feel normal again?
4
156
1,038
Neeja Bakshi
@NeejaB
·
13h
After 2.5 years, we have only begun to scratch the surface of Long COVID, and understand its impact on individuals. I fear we will continue to underestimate its impact on our province, our nation and truly the world. #LongCovid
34
223
1,466
Neeja Bakshi
@NeejaB
·
3h
Edited: thank you for the shares and the comments. Couple of common questions came up, I'll try to address, with the disclaimer that this is not medical advice, & while experiential medicine is important, I am very clear with my patients about risk vs benefit in any intervention.
1
7
172
Neeja Bakshi
@NeejaB
·
3h
1. What treatments am I recommending? If dysautonomia/POTS- common known tx: fluids, electrolytes, beta blockers, ivabradine (the latter often comes with cost / coverage barrier). Fatigue/inflammatory symptoms: antihistamines (Blexten, rupall); LDN (low dose naltrexone)
4
22
208
Neeja Bakshi
@NeejaB
·
3h
Other treatments usually based on symptoms - vitamin deficiency replacement, mood support (ADHD, depression), inhalers, anti-inflammatories, and much much more. Non pharmacological - rehabilitation (with the right team that understands CFS), acupuncture, counseling / CBT.
5
14
170
Neeja Bakshi
@NeejaB
·
3h
2. Vax vs unvaxxed - remember, this is a small sample size. Purely anecdotal. Those that got COVID in 2020 prior to vaccine being available (in my cohort) show far more debilitating and severe long COVID than those with even one dose. Vaccinated individuals can still get LC.
2
28
268
Neeja Bakshi
@NeejaB
·
3h
Unvaxxed appears to have worse symptomatology (again. Only in what I am seeing, this is not the same as a robust study that will be needed in general for LC).
1
13
189
Neeja Bakshi
@NeejaB
·
3h
3. This sounds like many other autoimmune, post-infectious syndromes that many suffer from: I agree. I am hopeful that that attention being given to LC, the subsequent research and treatment guidelines - will help a far larger population of patients who have been ill for so long.
- Do not take medical advice from the internet. If you have any medical questions please consult your medical practitioner.
LATEST POSTS - click HERE
Check out the FAQ,Terms of Service & Disclaimers by clicking the link. Please register to be able to post. By viewing this site you are agreeing to our Terms of Service and Acknowledge our Disclaimers.
FluTrackers.com Inc. does not provide medical advice. Information on this web site is collected from various internet resources, and the FluTrackers board of directors makes no warranty to the safety, efficacy, correctness or completeness of the information posted on this site by any author or poster. The information collated here is for instructional and/or discussion purposes only and is NOT intended to diagnose or treat any disease, illness, or other medical condition. Every individual reader or poster should seek advice from their personal physician/healthcare practitioner before considering or using any interventions that are discussed on this website. By continuing to access this website you agree to consult your personal physican before using any interventions posted on this website, and you agree to hold harmless FluTrackers.com Inc., the board of directors, the members, and all authors and posters for any effects from use of any medication, supplement, vitamin or other substance, device, intervention, etc. mentioned in posts on this website, or other internet venues referenced in posts on this website.- We are not asking for any donations. Do not donate to any entity who says they are raising funds for us.

Leave a comment: