 Tweet
Tweet
hat tip Ian Mackay
SATURDAY, 30 JANUARY 2016
Microcephaly in Brazil: is it occurring in greater numbers than normal or not?
A paper came out yesterday (AEST) from Morbidity and Mortality Weekly Report (MMWR) with the heading...
Reads as though some great data may finally show us a hint of an association between Zika virus (ZIKV) infection and microcephaly disease. Right?
Nope. There are none. At least none that could approach satisfying that title which highlights that it is not just the popular media who can generate misleading titles (headlines in their case).
In fact there are no Zika virus testing results in this study of 35 infants with microcephaly (defined using a useful protocol described detailed within). At all.
The closest we get to identifying a role for ZIKV in this disease are the statements...
"because Zika virus infection was not laboratory confirmed in infants or their mothers, the history of a nonspecific rash illness during pregnancy is subject to recall bias and might have resulted in misclassification of potential Zika virus exposure"
Recall bias being that thing you get when you don't really remember what happened a while ago; the details get a little hazy. I imagine that might be a factor in at least some instances here. But clearly not all.
The authors also note that the case definition they describe is unlikely to have been used prior to November 2015. For example, head measurement was not being routinely recorded thus milder cases may not have been reported prior to the ZIKV epidemic/pandemic/global epidemic/multi-country outbreak (or whatever it is being called-my choice underlined). Again, this doesn't negate the rise nor the issue, but it may reduce the total a little. This idea was given more oxygen earlier in the week in an article by Declan Butler in Nature.[4] Although not all agree, some even suggesting the numbers are underestimates.[5]
A little over a week ago I wondered why the United States had a higher averaged number of microcephaly cases than Brazil...
Flu-blog-eyah's ProfCrof has just penned a very nice analysis of this issue.[6]
He looks more deeply than I did and folks, this is why we should demand and ensure public health infectious disease data are accessible to the public-not all useful ideas come from, or are communicated by, a paid position.
The wash-up of Crof's analysis is that perhaps the rise in microcephaly cases is not a rise at all, but simply a more successful effort to collect data, and that the total number of microcephalic babies may not be too far from the norm (also considering those issues above).[6]
The MMWR study did look for, and found no evidence of the following infections of diseases...
So the MMWR paper is essentially providing a useful definition of microcephaly and informing us that a cohort has been started/is still recruiting (?) For me, its title would have been better written as
"Case definition of microcephaly epidemic in Brazil"or perhaps,
">insert name< : a birth cohort study into ZIKV infection and congenital disease"...or something.
 The search for a cause for Brazil's reported spike in microcephaly cases will go on. If it is a true spike then it must, but even that is not clear right now. As is much at all about ZIKV. This event in the Americas really serves a s reminder that we must keep our eyes open to all possibilities - we can do, and think, about more than one thing at a time. If it is not a true spike, then an awful lot of resources are currently moving towards defeating ZIKV that probably, sadly, would not be moving if microcephaly was not a front page story. Right now it seems we're not very clear on even the most basic facts.
The search for a cause for Brazil's reported spike in microcephaly cases will go on. If it is a true spike then it must, but even that is not clear right now. As is much at all about ZIKV. This event in the Americas really serves a s reminder that we must keep our eyes open to all possibilities - we can do, and think, about more than one thing at a time. If it is not a true spike, then an awful lot of resources are currently moving towards defeating ZIKV that probably, sadly, would not be moving if microcephaly was not a front page story. Right now it seems we're not very clear on even the most basic facts.
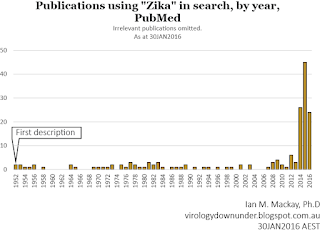
It is great to see some more papers coming out because there have not been many to date (see graph above). Bravo. It would be greater still if they had more relevant data and came out faster.
As always, don't just believe the headline. Read further. And maybe do your own analysis, like the Crof did.
References...
SATURDAY, 30 JANUARY 2016
Microcephaly in Brazil: is it occurring in greater numbers than normal or not?
A paper came out yesterday (AEST) from Morbidity and Mortality Weekly Report (MMWR) with the heading...
Possible Association Between Zika Virus Infection and Microcephaly — Brazil, 2015
Reads as though some great data may finally show us a hint of an association between Zika virus (ZIKV) infection and microcephaly disease. Right?
Nope. There are none. At least none that could approach satisfying that title which highlights that it is not just the popular media who can generate misleading titles (headlines in their case).
In fact there are no Zika virus testing results in this study of 35 infants with microcephaly (defined using a useful protocol described detailed within). At all.
The closest we get to identifying a role for ZIKV in this disease are the statements...
- "Therefore a mother’s report of a rash illness during pregnancy was used as a proxy indicator of potential Zika virus infection."
ZIKV is not the only agent capable of causing a rash-we've seen evidence for concurrent circulation of other rash-causing arboviruses in print from Brazil including dengue virus and chikungunya virus.[2] There is also malaria, filiaris, leishmaniasis and yellow fever to consider in this region.[3] - [cerebrospinal fluid] "CSF samples from all infants enrolled in the cohort were sent to a reference laboratory in Brazil for Zika virus testing; the results are not yet available."
Why publish these data ahead of these CSF results I wonder? It does not take long to perform RT-PCR for ZIKV. Certainly not long enough to hold up a paper for more than a day or two at most
"because Zika virus infection was not laboratory confirmed in infants or their mothers, the history of a nonspecific rash illness during pregnancy is subject to recall bias and might have resulted in misclassification of potential Zika virus exposure"
Recall bias being that thing you get when you don't really remember what happened a while ago; the details get a little hazy. I imagine that might be a factor in at least some instances here. But clearly not all.
The authors also note that the case definition they describe is unlikely to have been used prior to November 2015. For example, head measurement was not being routinely recorded thus milder cases may not have been reported prior to the ZIKV epidemic/pandemic/global epidemic/multi-country outbreak (or whatever it is being called-my choice underlined). Again, this doesn't negate the rise nor the issue, but it may reduce the total a little. This idea was given more oxygen earlier in the week in an article by Declan Butler in Nature.[4] Although not all agree, some even suggesting the numbers are underestimates.[5]
A little over a week ago I wondered why the United States had a higher averaged number of microcephaly cases than Brazil...

Flu-blog-eyah's ProfCrof has just penned a very nice analysis of this issue.[6]
He looks more deeply than I did and folks, this is why we should demand and ensure public health infectious disease data are accessible to the public-not all useful ideas come from, or are communicated by, a paid position.
The wash-up of Crof's analysis is that perhaps the rise in microcephaly cases is not a rise at all, but simply a more successful effort to collect data, and that the total number of microcephalic babies may not be too far from the norm (also considering those issues above).[6]
The MMWR study did look for, and found no evidence of the following infections of diseases...
- syphilis
- toxoplasmosis
- rubella
- cytomegalovirus
- herpes simplex virus
So the MMWR paper is essentially providing a useful definition of microcephaly and informing us that a cohort has been started/is still recruiting (?) For me, its title would have been better written as
"Case definition of microcephaly epidemic in Brazil"or perhaps,
">insert name< : a birth cohort study into ZIKV infection and congenital disease"...or something.
 The search for a cause for Brazil's reported spike in microcephaly cases will go on. If it is a true spike then it must, but even that is not clear right now. As is much at all about ZIKV. This event in the Americas really serves a s reminder that we must keep our eyes open to all possibilities - we can do, and think, about more than one thing at a time. If it is not a true spike, then an awful lot of resources are currently moving towards defeating ZIKV that probably, sadly, would not be moving if microcephaly was not a front page story. Right now it seems we're not very clear on even the most basic facts.
The search for a cause for Brazil's reported spike in microcephaly cases will go on. If it is a true spike then it must, but even that is not clear right now. As is much at all about ZIKV. This event in the Americas really serves a s reminder that we must keep our eyes open to all possibilities - we can do, and think, about more than one thing at a time. If it is not a true spike, then an awful lot of resources are currently moving towards defeating ZIKV that probably, sadly, would not be moving if microcephaly was not a front page story. Right now it seems we're not very clear on even the most basic facts.It is great to see some more papers coming out because there have not been many to date (see graph above). Bravo. It would be greater still if they had more relevant data and came out faster.
As always, don't just believe the headline. Read further. And maybe do your own analysis, like the Crof did.
References...
- Possible Association Between Zika Virus Infection and Microcephaly — Brazil, 2015
http://www.cdc.gov/mmwr/volumes/65/wr/pdfs/mm6503e2.pdf - Dengue, chikungunya and Zika co-infection in a patient from Colombia
http://www.jiph.org/article/S1876-03...221-X/abstract - https://smartraveller.gov.au/countries/brazil
- http://www.nature.com/news/zika-viru...report-1.19259
- http://www.wsj.com/articles/the-braz...aly-1454109620
- http://crofsblogs.typepad.com/h5n1/2...o-find-it.html


 (721 ko)
(721 ko)
Comment