 Tweet
Tweet
[Source: European Centre for Disease Prevention and Control (ECDC), full page: (LINK). Edited.]
Epidemiological update: Middle East respiratory syndrome coronavirus (MERS-CoV)
30 Apr 2014
As of 30 April 2014, 424 cases of MERS-CoV have been reported globally, including 131 deaths. All cases have either occurred in the Middle East or have direct links to a primary case infected in the Middle East.
Middle East
Europe
Africa
Asia
_____
The primary case for each chain was infected in the Middle East, and local secondary transmission following importation was reported from the United Kingdom, France, and Tunisia.
The number of reported cases increased markedly in April 2014 (Figure 1) with 217 cases and 38 deaths. Between March 2013 and March 2014 the monthly average number of reported cases was 15.
_____
Figure 1. Distribution of confirmed cases of MERS-CoV by month of onset* and probable place of infection, March 2012 ? 30 April 2014 (n=424**)

Download Figure 1
______
In April 2014, four countries (Philippines, Greece, Malaysia and Egypt) notified imported cases from Arabian Peninsula (Figure 2).
______
Figure 2. Distribution of confirmed cases of MERS-CoV by reporting country, March 2012 ? 30 April 2014 (n=424)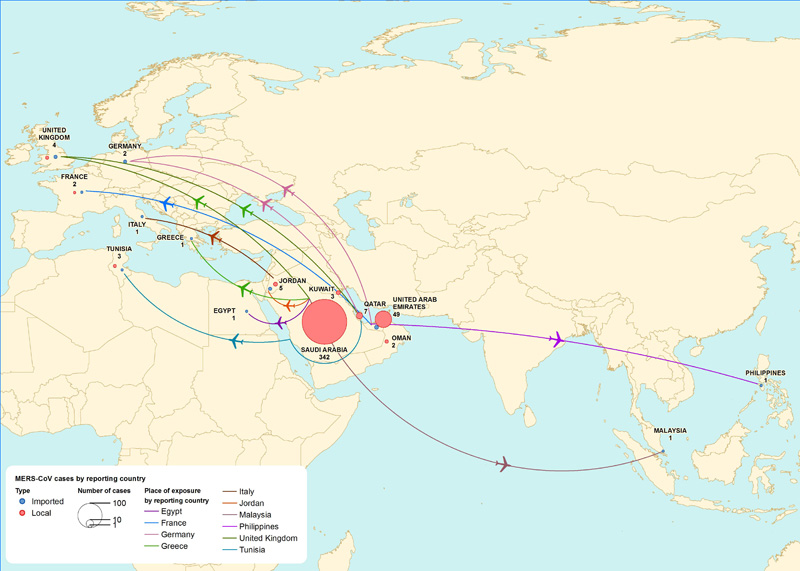
Download Figure 2
_______
As of 30 April 2014, the case-fatality ratio is 31 %.
The male to female ratio is 2:1.
Among the 419 cases with known age, the mean age is 49 years.
Median age was 50 (range 1-94 years) and 393 (94%) were older than 19 years.
Out of the 349 cases for whom age and sex is known, 177 (51%) have been males aged 40 years and above.
_______
Figure 3. Distribution of confirmed cases of MERS-CoV by age and sex, March 2012 ? 31 March 2014 (n=206*) and 01 April - 30 April 2014 (n=143**)
Download Figure 3
______
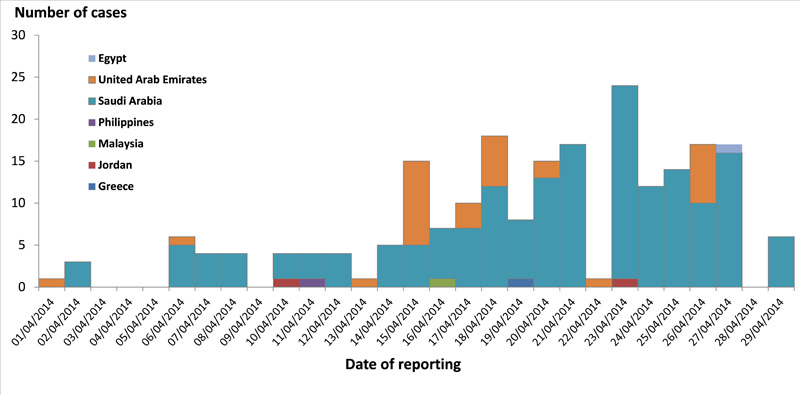
During April 2014, 217 cases were reported, as compared to the 207 cases reported from the beginning of the outbreak (March 2012) to 31 March 2014.
Among these 217 cases, 179 (82%) were reported by Saudi Arabia, 32 cases (15%) by the United Arab Emirates, 2 cases were reported by Jordan and one case each by Egypt, Greece, Malaysia and Philippines (Figure 4).
______
Figure 4. Distribution of confirmed cases of MERS-CoV by reporting country, 1 ? 30 April 2014 (n=217)
Download Figure 4
_______
Healthcare workers have been more frequently reported during the month of April 2014 than previously.
Since April 2012, 95 cases have been healthcare workers, of whom 62 (65%) were reported in April 2014.
Seventy (74%) of the healthcare workers were reported from Saudi Arabia, twenty-three (24%) from the United Arab Emirates, and one each from Philippines and Jordan.
The cause of the rapid increase in cases in April is unknown. The Rapid Risk Assessment of 24 April considers the possible scenarios that might explain this, notably:
On 26 April, Christian Drosten of Bonn University published a report in ProMed describing the preliminary results from sequence analysis of three viruses recovered from recent cases. These results suggest that the virus has not undergone major genetic changes compared to MERS/CoV sequenced earlier in the outbreak. The report also provide evidence against the hypothesis of a laboratory contamination causing this increase in reported cases.
ECDC continues to monitor information on the situation on MERS-CoV worldwide. In earlier Rapid Risk Assessments, ECDC concluded that the risk of importation of MERS-CoV to the EU was expected to continue and the risk of secondary transmission in the EU remains low. The assessment provided in the ECDC Rapid Risk Assessment on 24 April 2014 remains valid.
-
-------
Epidemiological update: Middle East respiratory syndrome coronavirus (MERS-CoV)
30 Apr 2014
As of 30 April 2014, 424 cases of MERS-CoV have been reported globally, including 131 deaths. All cases have either occurred in the Middle East or have direct links to a primary case infected in the Middle East.
Middle East
- Saudi Arabia: 342 cases / 105 deaths
- United Arab Emirates: 49 cases / 9 deaths
- Qatar: 7 cases / 4 deaths
- Jordan: 5 cases / 3 deaths
- Oman: 2 cases / 2 deaths
- Kuwait: 3 cases / 1 death
- Egypt: 1 case/ 0 deaths
Europe
- UK: 4 cases / 3 deaths
- Germany: 2 cases / 1 death
- France: 2 cases / 1 death
- Italy: 1 case / 0 deaths
- Greece: 1 case/ 0 deaths
Africa
- Tunisia: 3 cases / 1 death
Asia
- Malaysia: 1 case / 1 death
- Philippines: 1 case / 0 deaths
_____
The primary case for each chain was infected in the Middle East, and local secondary transmission following importation was reported from the United Kingdom, France, and Tunisia.
The number of reported cases increased markedly in April 2014 (Figure 1) with 217 cases and 38 deaths. Between March 2013 and March 2014 the monthly average number of reported cases was 15.
_____
Figure 1. Distribution of confirmed cases of MERS-CoV by month of onset* and probable place of infection, March 2012 ? 30 April 2014 (n=424**)
Download Figure 1
______
In April 2014, four countries (Philippines, Greece, Malaysia and Egypt) notified imported cases from Arabian Peninsula (Figure 2).
______
Figure 2. Distribution of confirmed cases of MERS-CoV by reporting country, March 2012 ? 30 April 2014 (n=424)
Download Figure 2
_______
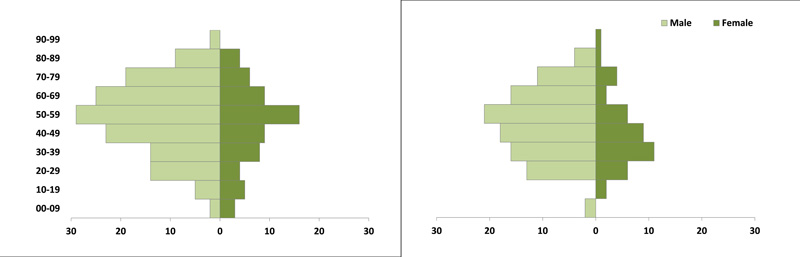
As of 30 April 2014, the case-fatality ratio is 31 %.
The male to female ratio is 2:1.
Among the 419 cases with known age, the mean age is 49 years.
Median age was 50 (range 1-94 years) and 393 (94%) were older than 19 years.
Out of the 349 cases for whom age and sex is known, 177 (51%) have been males aged 40 years and above.
_______
Figure 3. Distribution of confirmed cases of MERS-CoV by age and sex, March 2012 ? 31 March 2014 (n=206*) and 01 April - 30 April 2014 (n=143**)
Download Figure 3
______
During April 2014, 217 cases were reported, as compared to the 207 cases reported from the beginning of the outbreak (March 2012) to 31 March 2014.
Among these 217 cases, 179 (82%) were reported by Saudi Arabia, 32 cases (15%) by the United Arab Emirates, 2 cases were reported by Jordan and one case each by Egypt, Greece, Malaysia and Philippines (Figure 4).
______
Figure 4. Distribution of confirmed cases of MERS-CoV by reporting country, 1 ? 30 April 2014 (n=217)
Download Figure 4
_______
Healthcare workers have been more frequently reported during the month of April 2014 than previously.
Since April 2012, 95 cases have been healthcare workers, of whom 62 (65%) were reported in April 2014.
Seventy (74%) of the healthcare workers were reported from Saudi Arabia, twenty-three (24%) from the United Arab Emirates, and one each from Philippines and Jordan.
The cause of the rapid increase in cases in April is unknown. The Rapid Risk Assessment of 24 April considers the possible scenarios that might explain this, notably:
- More sensitive case detection through more active case finding and contact tracing or changes in testing algorithms,
- Increased zoonotic transmission with subsequent transmission in healthcare settings,
- Breakdown in infection control measures or otherwise increased transmission in the local healthcare setting,
- Change in the virus resulting in more effective human-to-human transmission, resulting in both nosocomial clusters, and increased numbers of asymptomatic community acquired cases, or
- False positive lab results.
On 26 April, Christian Drosten of Bonn University published a report in ProMed describing the preliminary results from sequence analysis of three viruses recovered from recent cases. These results suggest that the virus has not undergone major genetic changes compared to MERS/CoV sequenced earlier in the outbreak. The report also provide evidence against the hypothesis of a laboratory contamination causing this increase in reported cases.
ECDC continues to monitor information on the situation on MERS-CoV worldwide. In earlier Rapid Risk Assessments, ECDC concluded that the risk of importation of MERS-CoV to the EU was expected to continue and the risk of secondary transmission in the EU remains low. The assessment provided in the ECDC Rapid Risk Assessment on 24 April 2014 remains valid.
-
-------