 Tweet
Tweet
UK NERVTAG Report On Immunity After Natural COVID Infection
#16,015
Fourteen months ago - literally within a few weeks of the declaration of the COVID pandemic, and long before variants were part of the equation - we were looking at concerns over the the reinfection potential of SARS-CoV-2 (see COVID-19: From Here To Immunity).
The notion that once infected and recovered (or eventually vaccinated) you'd be immune for life was based on other viral diseases like mumps and measles, even though we've seen plenty of evidence of other viral infections - including coronaviruses- having a less than permanent impact on the human immune system.
Early reports of reinfections were dismissed as more likely relapses, or failures in testing, but by late summer we began to see a small number of laboratory confirmed reinfections around the globe (see Another SARS-COV-2 Reinfection Report To Ponder (Nevada, United States).
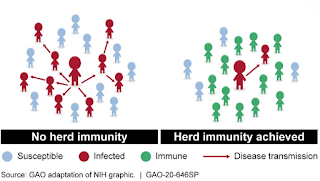
Herd immunity took another hit in December 2020, when Brazil - whose population had already seen a massive spring wave and was assumed to be largely immune to another wave - was hit by the P.1 variant, causing their biggest epidemic to date (see The Lancet: Resurgence of COVID-19 in Manaus, Brazil, Despite High Seroprevalence).
While relatively rare in 2020 - between the rise and global spread of multiple variants, and the passage of time - the risk of reinfection (or vaccine breakthrough), has grown markedly over the few months.
That said, most people who have been previously infected (or vaccinated) appear to retain significant levels of immunity against SARS-CoV-2 even after 6 months, although immunity varies considerably by the individual.
For some, protection may last for years to come, while for others, their defensive shields may already be down.
A population based study out of Denmark publish in March 2021 (see Denmark SSI: Assessment of Protection Against Reinfection with SARS-CoV-2) found that those under 65 are about 80% protected - at in the short term (6 months) - against reinfection with COVID-19.
Among those aged 65 and over, however, that protection is estimated to be only 47%.
It should be noted that these results were based primarily on the older, `wild type' COVID, not the recently emerged variants carrying the E484K mutation, and so these numbers may not hold true going forward.
To better understand (and identify) COVID reinfections, in April the ECDC released a 10-page Technical Rpt: Reinfection with SARS-CoV-2 , with case definitions and testing requirements.
To this ongoing saga we can add a new report from the UK's NERVTAG(New and Emerging Respiratory Virus Threats Advisory Group) that attempts to quantify - based on growing, but still incomplete information - the amount of immunity people may have following natural infection with COVID-19.
While COVID infection appears to leave behind significant community immunity even 8 months post infection, not everyone comes away with the same high level of protection.
Citing a low confidence level, this report finds roughly half of those over 65 may be vulnerable to reinfection, while they more confidently submit that close to 20% of the rest of the population may be susceptible to symptomatic reinfection within the first 7 months.
They also warn that: Protection against SARS-CoV-2 infection, disease, and transmission may be diminished by antigenic changes in variant viruses (high confidence).
I've only reproduced the summary and conclusion sections of this 14-page report. Follow the link to read it in its entirety.
Update note on immunity to SARS-CoV-2 after natural infection
Authors: Peter Openshaw, Catherine Huntley, Peter Horby, Wendy Barclay, Andrew Hayward
Acknowledgements: M. K. Siggins, R. S. Thwaites and P. J. Openshaw, “Durability of Immunity to SARS-CoV-2 and Other Respiratory Viruses,” Trends in Microbiology, 2021 (ref.22 of this document) acted as a source for this summary.
27 th May 2021
Summary
1. Most people infected with SARS-CoV-2 generate an antibody response in serum, saliva and mucosal fluids within 1–3 weeks after symptom onset. However, there is heterogeneity, some with mild disease developing weak antibody responses.
2. Antibody is detectable in saliva for at least 8 months, and in blood for at least 9 months after infection (high confidence) but individual trajectories vary and levels depend on the assay method (of which there are many).
3. Cells making antibody (plasma cells) or with the capacity to rapidly make antibody (memory B cells) can be detected up to 8 months after infection.
4. Most convalescent individuals show T cell responses to SARS-CoV-2 after infection, that can be detected for at least 8 months. However, activated virus-specific T cells are only transiently present in the peripheral circulation at measurable levels and thereafter need to be recovered by restimulation in vitro. T cells have antiviral effects on contact with infected cells, but not when circulating free in the blood.
5. Memory B cells and specific T cells enhance long-term protection against severe COVID-19 caused by current and (to a lesser extent) future variants of SARS-CoV-2.
6. These immune responses lessen disease severity (high confidence) but may also reduce viral replication in the respiratory mucosa and inhibit SARS-CoV-2 transmission (moderate confidence).
7. Following natural infection with SARS-CoV-2:
a. Protection against symptomatic PCR-confirmed infection with SARS-CoV-2 is high for a period of at least 7 months, estimated at 81% (95% CI 75-84%) (high confidence).
b. Protection against all PCR-confirmed infections with SARS-CoV-2 is high for a period of at least 6 months, estimated to be 69% (95%CI – 60-76%) (high confidence).
c. Protection against asymptomatic or atypical PCR-confirmed infections with SARS-CoV-2 is moderate for a period of at least 6 months, estimated at 40% (95% CI 20-55%) (high confidence).
d. Protective effectiveness against symptomatic PCR-confirmed infection in those aged over 65 is lower than in younger age groups, estimated at 47.1% (95%CI 24.7-62.8%) (low confidence).
8. Protection against SARS-CoV-2 infection, disease, and transmission may be diminished by antigenic changes in variant viruses (high confidence).
(SNIP)
(Continue . . . )

#16,015
Fourteen months ago - literally within a few weeks of the declaration of the COVID pandemic, and long before variants were part of the equation - we were looking at concerns over the the reinfection potential of SARS-CoV-2 (see COVID-19: From Here To Immunity).
The notion that once infected and recovered (or eventually vaccinated) you'd be immune for life was based on other viral diseases like mumps and measles, even though we've seen plenty of evidence of other viral infections - including coronaviruses- having a less than permanent impact on the human immune system.
Early reports of reinfections were dismissed as more likely relapses, or failures in testing, but by late summer we began to see a small number of laboratory confirmed reinfections around the globe (see Another SARS-COV-2 Reinfection Report To Ponder (Nevada, United States).
Herd immunity took another hit in December 2020, when Brazil - whose population had already seen a massive spring wave and was assumed to be largely immune to another wave - was hit by the P.1 variant, causing their biggest epidemic to date (see The Lancet: Resurgence of COVID-19 in Manaus, Brazil, Despite High Seroprevalence).
While relatively rare in 2020 - between the rise and global spread of multiple variants, and the passage of time - the risk of reinfection (or vaccine breakthrough), has grown markedly over the few months.
That said, most people who have been previously infected (or vaccinated) appear to retain significant levels of immunity against SARS-CoV-2 even after 6 months, although immunity varies considerably by the individual.
For some, protection may last for years to come, while for others, their defensive shields may already be down.
A population based study out of Denmark publish in March 2021 (see Denmark SSI: Assessment of Protection Against Reinfection with SARS-CoV-2) found that those under 65 are about 80% protected - at in the short term (6 months) - against reinfection with COVID-19.
Among those aged 65 and over, however, that protection is estimated to be only 47%.
It should be noted that these results were based primarily on the older, `wild type' COVID, not the recently emerged variants carrying the E484K mutation, and so these numbers may not hold true going forward.
To better understand (and identify) COVID reinfections, in April the ECDC released a 10-page Technical Rpt: Reinfection with SARS-CoV-2 , with case definitions and testing requirements.
To this ongoing saga we can add a new report from the UK's NERVTAG(New and Emerging Respiratory Virus Threats Advisory Group) that attempts to quantify - based on growing, but still incomplete information - the amount of immunity people may have following natural infection with COVID-19.
While COVID infection appears to leave behind significant community immunity even 8 months post infection, not everyone comes away with the same high level of protection.
Citing a low confidence level, this report finds roughly half of those over 65 may be vulnerable to reinfection, while they more confidently submit that close to 20% of the rest of the population may be susceptible to symptomatic reinfection within the first 7 months.
They also warn that: Protection against SARS-CoV-2 infection, disease, and transmission may be diminished by antigenic changes in variant viruses (high confidence).
I've only reproduced the summary and conclusion sections of this 14-page report. Follow the link to read it in its entirety.
Update note on immunity to SARS-CoV-2 after natural infection
Authors: Peter Openshaw, Catherine Huntley, Peter Horby, Wendy Barclay, Andrew Hayward
Acknowledgements: M. K. Siggins, R. S. Thwaites and P. J. Openshaw, “Durability of Immunity to SARS-CoV-2 and Other Respiratory Viruses,” Trends in Microbiology, 2021 (ref.22 of this document) acted as a source for this summary.
27 th May 2021
Summary
1. Most people infected with SARS-CoV-2 generate an antibody response in serum, saliva and mucosal fluids within 1–3 weeks after symptom onset. However, there is heterogeneity, some with mild disease developing weak antibody responses.
2. Antibody is detectable in saliva for at least 8 months, and in blood for at least 9 months after infection (high confidence) but individual trajectories vary and levels depend on the assay method (of which there are many).
3. Cells making antibody (plasma cells) or with the capacity to rapidly make antibody (memory B cells) can be detected up to 8 months after infection.
4. Most convalescent individuals show T cell responses to SARS-CoV-2 after infection, that can be detected for at least 8 months. However, activated virus-specific T cells are only transiently present in the peripheral circulation at measurable levels and thereafter need to be recovered by restimulation in vitro. T cells have antiviral effects on contact with infected cells, but not when circulating free in the blood.
5. Memory B cells and specific T cells enhance long-term protection against severe COVID-19 caused by current and (to a lesser extent) future variants of SARS-CoV-2.
6. These immune responses lessen disease severity (high confidence) but may also reduce viral replication in the respiratory mucosa and inhibit SARS-CoV-2 transmission (moderate confidence).
7. Following natural infection with SARS-CoV-2:
a. Protection against symptomatic PCR-confirmed infection with SARS-CoV-2 is high for a period of at least 7 months, estimated at 81% (95% CI 75-84%) (high confidence).
b. Protection against all PCR-confirmed infections with SARS-CoV-2 is high for a period of at least 6 months, estimated to be 69% (95%CI – 60-76%) (high confidence).
c. Protection against asymptomatic or atypical PCR-confirmed infections with SARS-CoV-2 is moderate for a period of at least 6 months, estimated at 40% (95% CI 20-55%) (high confidence).
d. Protective effectiveness against symptomatic PCR-confirmed infection in those aged over 65 is lower than in younger age groups, estimated at 47.1% (95%CI 24.7-62.8%) (low confidence).
8. Protection against SARS-CoV-2 infection, disease, and transmission may be diminished by antigenic changes in variant viruses (high confidence).
(SNIP)
Conclusions
57. Infection with SARS-CoV-2 leads to antibody, B cell, and T cell responses in almost all individuals, which are sustained for over 8 months after infection (high confidence).
58. Virus-specific IgA and tissue-resident T cells provide mucosal protection against SARSCoV-2 but may have limited duration (moderate confidence).
59. Neutralising antibodies to SARS-CoV-2 can lead to sterilising immunity, and measurement of antibodies against RBD or S1 using robust serological assays is likely to correlate with protection against natural exposure to SARS-CoV-2 (moderate confidence).
60. Data from other respiratory viruses suggest that a combination of neutralising antibodies produced by long-lived plasma cells, and immunological support from memory B and T cells, can provide long-term protection against severe disease (high confidence).
61. Data are insufficient to assess the impact of natural immunity on transmission, though the presence of neutralising antibody is associated with a reduction in shedding of infectious virus (moderate confidence).
62. Immunity against SARS-CoV-2 infection may be diminished by viral evolution and the emergence of variants (high confidence).
63. Disease attenuating (functional) immunity is more likely to be maintained long-term than sterilising immunity because lower levels of immunity are needed to attenuate severity as opposed to preventing infection (moderate confidence)
57. Infection with SARS-CoV-2 leads to antibody, B cell, and T cell responses in almost all individuals, which are sustained for over 8 months after infection (high confidence).
58. Virus-specific IgA and tissue-resident T cells provide mucosal protection against SARSCoV-2 but may have limited duration (moderate confidence).
59. Neutralising antibodies to SARS-CoV-2 can lead to sterilising immunity, and measurement of antibodies against RBD or S1 using robust serological assays is likely to correlate with protection against natural exposure to SARS-CoV-2 (moderate confidence).
60. Data from other respiratory viruses suggest that a combination of neutralising antibodies produced by long-lived plasma cells, and immunological support from memory B and T cells, can provide long-term protection against severe disease (high confidence).
61. Data are insufficient to assess the impact of natural immunity on transmission, though the presence of neutralising antibody is associated with a reduction in shedding of infectious virus (moderate confidence).
62. Immunity against SARS-CoV-2 infection may be diminished by viral evolution and the emergence of variants (high confidence).
63. Disease attenuating (functional) immunity is more likely to be maintained long-term than sterilising immunity because lower levels of immunity are needed to attenuate severity as opposed to preventing infection (moderate confidence)
(Continue . . . )
Comment