 Tweet
Tweet
UK: NERVTAG paper on COVID-19 variant of concern B.1.1.7

UK PM Boris Johnson Press Conference today Jan 22nd
#15,737
With the caveat that this data is preliminary, and more analysis is needed - the news that the B.1.1.7 (aka `UK') variant might carry a higher fatality rate than the `wild type' COVID virus broke in the British media earlier today - and was confirmed by UK Prime Minister Boris Johnson a couple of hours ago in a press conference.
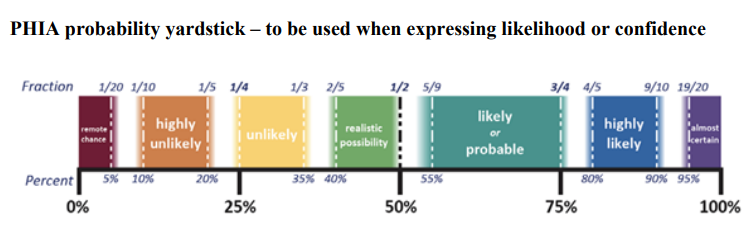
This announcement is based on the findings of a NERVTAG report, which finds there is a realistic possibility that VOC B.1.1.7 is associated with an increased risk of death compared to non-VOC viruses. That increased risk appears at this time to be about 30%.
A `Realistic Possibility' is defined by the scale below as somewhere between a 40% and 50% confidence level. So this is far from a foregone conclusion.

The UK"s Department of Health and Social Care has posted the NERVTAG report (see below), which provides the basis for this announcement. First the link to the report, and a brief summary, followed by some excerpts.
Excerpts from the 8-page report follow:
NERVTAG Summary
1. The variant of concern (VOC) B.1.1.7 appears to have substantially increased transmissibility compared to other variants and has grown quickly to become the dominant variant in much of the UK.
2. Initial assessment by PHE of disease severity through a matched case-control study reported no significant difference in the risk of hospitalisation or death in people infected with confirmed B.1.1.7 infection versus infection with other variants. [1]
3. Several new analyses are however consistent in reporting increased disease severity in people infected with VOC B.1.1.7 compared to people infected with non-VOC virus variants.
4. There have been several independent analyses of SGTF and non-SGTF cases identified through Pillar 2 testing linked to the PHE COVID-19 deaths line list:
5. An updated PHE matched cohort analysis has reported a death risk ratio for VOC infected individuals compared to non-VOC of 1.65 (95%CI 1.21-2.25)
6. There are several limitations to these datasets including representativeness of death data (<10% of all deaths are included in some datasets), power, potential biases in case ascertainment and transmission setting.
7. Based on these analyses, there is a realistic possibility that infection with VOC B.1.1.7 is associated with an increased risk of death compared to infection with non-VOC viruses.
8. It should be noted that the absolute risk of death per infection remains low.
9. An analysis of CO-CIN data has not identified an increased risk of death in hospitalised VOC B.1.1.7 cases. However, increased severity may not necessarily be reflected by increased in-hospital death risk.
10. Since the time lag from infection to hospitalisation and death is relatively long, data will accrue in coming weeks, at which time the analyses will become more definitive.
(Continue . . . )
While it may take a few weeks to truly pin down these numbers, this is a reminder that viruses can change abruptly, and that past performance is no guarantee of future results.
UK PM Boris Johnson Press Conference today Jan 22nd
#15,737
With the caveat that this data is preliminary, and more analysis is needed - the news that the B.1.1.7 (aka `UK') variant might carry a higher fatality rate than the `wild type' COVID virus broke in the British media earlier today - and was confirmed by UK Prime Minister Boris Johnson a couple of hours ago in a press conference.
This announcement is based on the findings of a NERVTAG report, which finds there is a realistic possibility that VOC B.1.1.7 is associated with an increased risk of death compared to non-VOC viruses. That increased risk appears at this time to be about 30%.
A `Realistic Possibility' is defined by the scale below as somewhere between a 40% and 50% confidence level. So this is far from a foregone conclusion.
The UK"s Department of Health and Social Care has posted the NERVTAG report (see below), which provides the basis for this announcement. First the link to the report, and a brief summary, followed by some excerpts.
NERVTAG paper on COVID-19 variant of concern B.1.1.7- PDF, 141KB, 8 pages
Some preliminary analyses have been undertaken which show that there may be an increase in the severity of disease associated with this new variant, B.1.1.7.
There are some important limitations to the data on which these analyses are based. A relatively small number of people were included in the analyses and from a small number of settings, so more data is being collected and the position will become clearer over the coming weeks.
Some preliminary analyses have been undertaken which show that there may be an increase in the severity of disease associated with this new variant, B.1.1.7.
There are some important limitations to the data on which these analyses are based. A relatively small number of people were included in the analyses and from a small number of settings, so more data is being collected and the position will become clearer over the coming weeks.
Excerpts from the 8-page report follow:
NERVTAG Summary
1. The variant of concern (VOC) B.1.1.7 appears to have substantially increased transmissibility compared to other variants and has grown quickly to become the dominant variant in much of the UK.
2. Initial assessment by PHE of disease severity through a matched case-control study reported no significant difference in the risk of hospitalisation or death in people infected with confirmed B.1.1.7 infection versus infection with other variants. [1]
3. Several new analyses are however consistent in reporting increased disease severity in people infected with VOC B.1.1.7 compared to people infected with non-VOC virus variants.
4. There have been several independent analyses of SGTF and non-SGTF cases identified through Pillar 2 testing linked to the PHE COVID-19 deaths line list:
a. LSHTM: reported that the relative hazard of death within 28 days of test for VOC-infected individuals compared to non-VOC was 1.35 (95%CI 1.08-1.68).
b. Imperial College London: mean ratio of CFR for VOC-infected individuals compared to non-VOC was 1.36 (95%CI 1.18-1.56) by a case-control weighting method, 1.29 (95%CI 1.07-1.54) by a standardised CFR method.
c. University of Exeter: mortality hazard ratio for VOC-infected individuals compared to non-VOC was 1.91 (1.35 - 2.71).
d. These analyses were all adjusted in various ways for age, location, time and other variables.
5. An updated PHE matched cohort analysis has reported a death risk ratio for VOC infected individuals compared to non-VOC of 1.65 (95%CI 1.21-2.25)
6. There are several limitations to these datasets including representativeness of death data (<10% of all deaths are included in some datasets), power, potential biases in case ascertainment and transmission setting.
7. Based on these analyses, there is a realistic possibility that infection with VOC B.1.1.7 is associated with an increased risk of death compared to infection with non-VOC viruses.
8. It should be noted that the absolute risk of death per infection remains low.
9. An analysis of CO-CIN data has not identified an increased risk of death in hospitalised VOC B.1.1.7 cases. However, increased severity may not necessarily be reflected by increased in-hospital death risk.
10. Since the time lag from infection to hospitalisation and death is relatively long, data will accrue in coming weeks, at which time the analyses will become more definitive.
(Continue . . . )
While it may take a few weeks to truly pin down these numbers, this is a reminder that viruses can change abruptly, and that past performance is no guarantee of future results.



Comment