 Tweet
Tweet
COVID-19: The Airborne Division

#15,171
More than 3 months after the novel coronavirus was first announced in Wuhan City, there is still sharp division among scientists whether SAR-CoV-2 - the virus that causes COVID-19 - is an `airborne' pathogen, or is spread primarily by large droplets.
This makes a huge practical difference, because the WHO - which subscribes to the `droplet' theory - only recommends `contact and droplet precautions' (gloves, gown, surgical mask & eye protection) for HCWs dealing with COVID-19 patients.
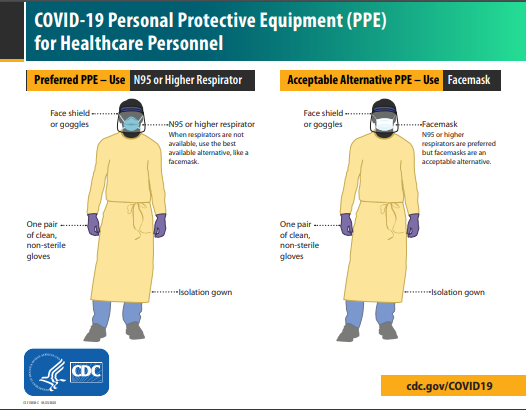
Many other scientists, however, aren't so certain. And getting this wrong, and recommending the wrong type of PPEs, could cost lives. In the United States, the CDC preferentially recommends N95s (when available), but due to shortages has proposed an `acceptable alternative'.
You can read about the current scientific debate over the airborne spread of COVID-19 in the following April 2nd article in Nature:
02 APRIL 2020
We all want evidence-based medicine and public health policies, but sometimes, the evidence is either scant or slow in coming. And for reasons that escape me, many officials seem to assume a threat is benign, until proven otherwise.
Lest we forget, it wasn't until January 18th - nearly 3 weeks after the Wuhan pneumonia outbreak became known outside of China - that the WHO finally reversed their `No evidence of Human-to-Human Transmission' mantra.
By that time, I think most of us had assumed H-2-H transmission was occuring, but even then the WHO was downplaying `sustained' transmission potential based on a lack of `clear evidence'.
Obviously, China had to know it was sustained and efficient by then, but that's a rant for another day . . .
I'm not a scientist, but as a paramedic, if I came across a car wreck with a downed electrical wire draped across the vehicle, I'm going to assume it is `hot' until proven otherwise.
I'll leave the definitive `two wet finger test' for someone else to perform.
This need for `clear evidence' or scientific certainty before making a decision or acting decisively isn't always practical in the real world, where weighing the evidence for days, weeks, or months can cost lives.
In 2014, two Texas nurses fell ill after treating an imported Ebola case, sparking a heated debate over the quality of both their PPEs and their safety training (see Nurses Claim Lack Of Safety Protocols For Dealing With Ebola).
At the time, the CDC's recommendations for HCWs dealing with a suspected or confirmed Ebola case included contact (gloves, gown) and droplet protection (surgical masks, eye protection), but full skin covering and the use of respirators (ie. PAPR, N95) were not advised for patient care not involving aerosol generating procedures (AGPs).
Five days later the CDC issued Stricter PPE Recommendations For Ebola, including:
The sound `scientific evidence' on October 15th was found wanting by the 20th. Looking back, it's hard to believe that surgical masks were ever deemed appropriate for Ebola.
While some may argue there isn't 100% proof that COVID-19 is airborne, or clear evidence that N95s would offer substantially superior protection to HCWs, it is hard not to assume the real reason behind the surgical mask recommendation is the global shortage of anything better.
Most HCWs realize this - and while feeling betrayed by this lack of preparedness - will probably soldier on with whatever PPEs they have. But by hiding behind this `lack of clear evidence' excuse, officials are only adding insult to potential injury.

#15,171
More than 3 months after the novel coronavirus was first announced in Wuhan City, there is still sharp division among scientists whether SAR-CoV-2 - the virus that causes COVID-19 - is an `airborne' pathogen, or is spread primarily by large droplets.
This makes a huge practical difference, because the WHO - which subscribes to the `droplet' theory - only recommends `contact and droplet precautions' (gloves, gown, surgical mask & eye protection) for HCWs dealing with COVID-19 patients.
Many other scientists, however, aren't so certain. And getting this wrong, and recommending the wrong type of PPEs, could cost lives. In the United States, the CDC preferentially recommends N95s (when available), but due to shortages has proposed an `acceptable alternative'.
You can read about the current scientific debate over the airborne spread of COVID-19 in the following April 2nd article in Nature:
02 APRIL 2020
Is the coronavirus airborne? Experts can’t agree
The World Health Organization says the evidence is not compelling, but scientists warn that gathering sufficient data could take years and cost lives.
The World Health Organization says the evidence is not compelling, but scientists warn that gathering sufficient data could take years and cost lives.
We all want evidence-based medicine and public health policies, but sometimes, the evidence is either scant or slow in coming. And for reasons that escape me, many officials seem to assume a threat is benign, until proven otherwise.
Lest we forget, it wasn't until January 18th - nearly 3 weeks after the Wuhan pneumonia outbreak became known outside of China - that the WHO finally reversed their `No evidence of Human-to-Human Transmission' mantra.
According to the latest information received and @WHO analysis, there is evidence of limited human-to-human transmission of #nCOV. This is in line with experience with other respiratory illnesses and in particular with other coronavirus outbreaks.
While there is currently no clear evidence of sustained human-to-human transmission, we do not have enough evidence to evaluate the full extent of human-to-human transmission. This is one of the issues that @WHO is monitoring closely.
By that time, I think most of us had assumed H-2-H transmission was occuring, but even then the WHO was downplaying `sustained' transmission potential based on a lack of `clear evidence'.
Obviously, China had to know it was sustained and efficient by then, but that's a rant for another day . . .
I'm not a scientist, but as a paramedic, if I came across a car wreck with a downed electrical wire draped across the vehicle, I'm going to assume it is `hot' until proven otherwise.
I'll leave the definitive `two wet finger test' for someone else to perform.
This need for `clear evidence' or scientific certainty before making a decision or acting decisively isn't always practical in the real world, where weighing the evidence for days, weeks, or months can cost lives.
In 2014, two Texas nurses fell ill after treating an imported Ebola case, sparking a heated debate over the quality of both their PPEs and their safety training (see Nurses Claim Lack Of Safety Protocols For Dealing With Ebola).
At the time, the CDC's recommendations for HCWs dealing with a suspected or confirmed Ebola case included contact (gloves, gown) and droplet protection (surgical masks, eye protection), but full skin covering and the use of respirators (ie. PAPR, N95) were not advised for patient care not involving aerosol generating procedures (AGPs).
Five days later the CDC issued Stricter PPE Recommendations For Ebola, including:
- No exposed skin
- N95 or PAPR instead of surgical or facemask
- Use of virocidal wipes on exterior of PPEs before doffing
The sound `scientific evidence' on October 15th was found wanting by the 20th. Looking back, it's hard to believe that surgical masks were ever deemed appropriate for Ebola.
While some may argue there isn't 100% proof that COVID-19 is airborne, or clear evidence that N95s would offer substantially superior protection to HCWs, it is hard not to assume the real reason behind the surgical mask recommendation is the global shortage of anything better.
Most HCWs realize this - and while feeling betrayed by this lack of preparedness - will probably soldier on with whatever PPEs they have. But by hiding behind this `lack of clear evidence' excuse, officials are only adding insult to potential injury.
Comment